

Choroidal thickness in older patients with central serous chorioretinopathy
- PMID: 27847640
- PMCID: PMC5088461
- DOI: 10.1186/s40942-016-0046-7
Choroidal thickness in older patients with central serous chorioretinopathy
Abstract
Background: To investigate the choroidal thickness in older patients with central serous chorioretinopathy (CSCR) compared to age-matched normal subjects.
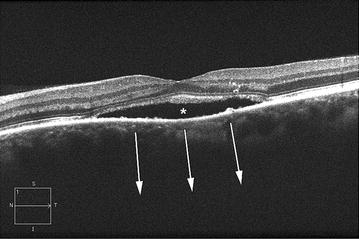
Methods: Fifteen patients (30 eyes) with CSCR, all aged ≥60 years, and 21 age-matched normal subjects (21 eyes) underwent high-definition raster scanning using SD-OCT. Both eyes from CSCR patients were included in the analysis. The eyes in patients with CSCR were divided into two groups: active CSCR (17 eyes) if there was foveal-involving subretinal fluid and inactive contralateral eye group (13 eyes). Choroidal thickness was measured from the posterior edge of the retinal pigment epithelium to the choroidal-scleral junction at 500 µm intervals up to 2500 µm temporal and nasal to the fovea (11 locations).
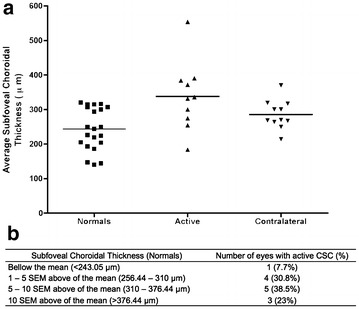
Results: The mean age of the patients with CSCR was 68.87 ± 6.83 years (mean ± standard deviation). Reliable measurements of choroidal thickness were obtainable in 70.6 % of eyes examined. The choroid was statistically significantly thicker in eyes with both active CSCR (P < 0.001) and inactive contralateral eyes (P < 0.01) when compared to normal age-matched eyes. The subfoveal choroid was 95 µm (P < 0.01) thicker in eyes with active CSCR (338.05 ± 31.42 µm) compared with normal eyes (243.05 ± 13.39 µm). The subfoveal choroid thickness in the inactive contralateral eyes was numerically greater than normal, and it was not statistically significantly thicker compared to the normal eyes (difference-55.68 µm, P > 0.05).
Conclusion: Choroid in older patients with active CSCR was thicker than the choroid in age-matched normal eyes. It is important to consider CSCR as a differential diagnosis of serous retinal detachment in elderly patients with thickened choroid and to consider SD-OCT as an imaging modality by which to evaluate the choroidal thickness.
Keywords: Central serous chorioretinopathy; Choroid; Optical coherence tomography.
Figures


References
-
- Hussain D, Gass JD. Idiopathic central serous chorioretinopathy. Indian J Ophthalmol. 1998;46(3):131–137. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
