

Clinical outcome and prognostic factors of patients with early-stage epithelial ovarian cancer
- PMID: 27852043
- PMCID: PMC5410350
- DOI: 10.18632/oncotarget.13317
Clinical outcome and prognostic factors of patients with early-stage epithelial ovarian cancer
Abstract
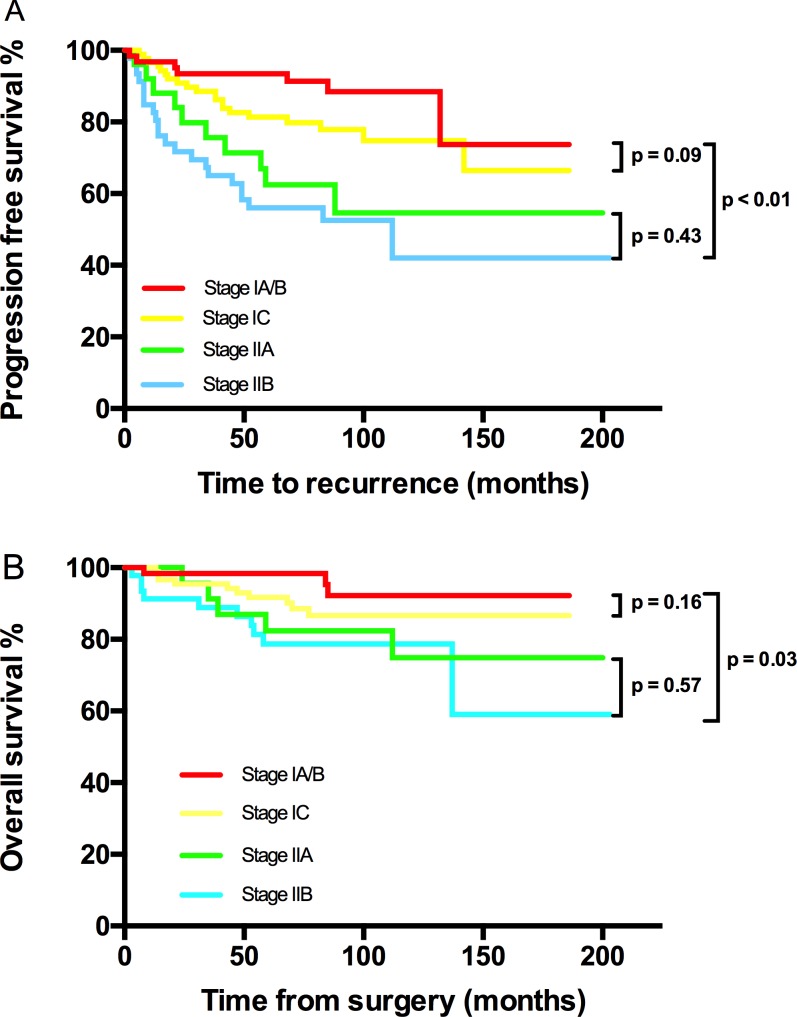
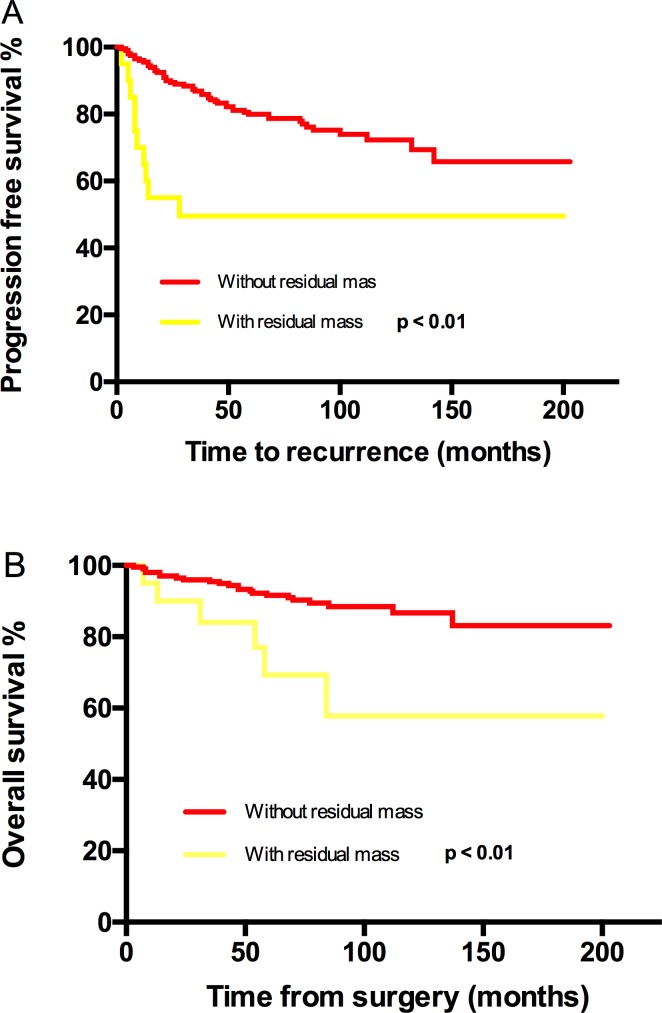
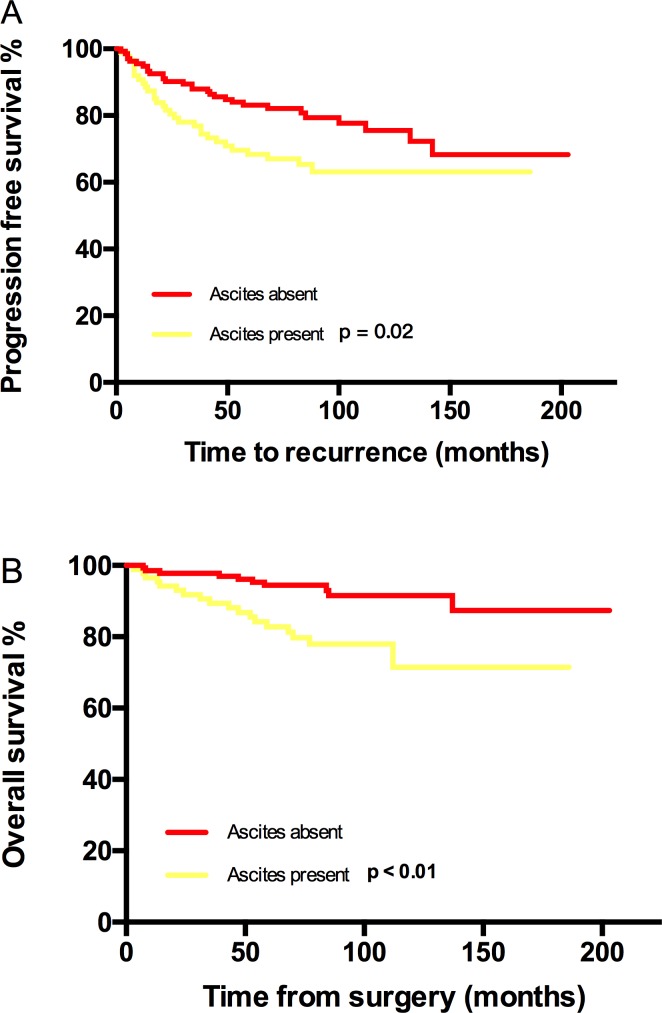
Some subsets of early stage ovarian cancer patients experience more recurrences than others. Studies on prognostics factors gave conflicting results. We investigated consecutive 221 patients with stage I/II ovarian cancer at our institution from 1999 to 2010. Univariate and multivariate analysis of progression free survival (PFS) and overall survival (OS) were performed. After a median follow-up of 79 months, the 5-year/10-year PFS and 5-year/10-year OS were 78% /76% and 90% /87% respectively. Multivariate analysis revealed that stage as the most prominent independent prognostic factor in terms of PFS (stage I vs stage IIA vs stage IIB, Hazard Ratio (HR): 1 vs 4 vs 6.1, P < 0.05) and OS (stage I vs stage II, HR: 1 vs 2.1, P < 0.05). Peritoneal biopsy reduced the risk of recurrence by 29% (95% CI: 0.15-0.58, P < 0.05). Ascites (HR = 2.8, 95% CI: 1.2-6.6, P < 0.05) and not the first-line chemotherapy (HR = 2.6, 95% CI: 1.1-6.5, P < 0.05) contributed to decreased OS. Overall, early-stage ovarian cancer had a favorable outcome, stage was the most powerful prognostic factor.
Keywords: early-stage; ovarian cancer; prognosis; recurrence; survival.
Conflict of interest statement
All Authors declare no conflicts of interest.
Figures
Similar articles
-
Glasgow prognostic score is an independent marker for poor prognosis with all cases of epithelial ovarian cancer.Cancer Med. 2016 Jun;5(6):1074-80. doi: 10.1002/cam4.681. Epub 2016 Mar 1. Cancer Med. 2016. PMID: 26929186 Free PMC article.
-
Comparison of early-stage primary serous fallopian tube carcinomas and equivalent stage serous epithelial ovarian carcinomas.Taiwan J Obstet Gynecol. 2014 Dec;53(4):547-51. doi: 10.1016/j.tjog.2014.06.002. Taiwan J Obstet Gynecol. 2014. PMID: 25510699
-
Secondary cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for recurrent epithelial ovarian cancer: a multi-institutional study.BJOG. 2012 Jun;119(7):800-9. doi: 10.1111/j.1471-0528.2011.03207.x. BJOG. 2012. PMID: 22571746
-
Dose-dense approaches to ovarian cancer treatment.Curr Treat Options Oncol. 2015 May;16(5):21. doi: 10.1007/s11864-015-0338-4. Curr Treat Options Oncol. 2015. PMID: 25859831 Review.
-
[Epithelial ovarian cancer - a change of paradigm].Ther Umsch. 2011 Oct;68(10):565-72. doi: 10.1024/0040-5930/a000215. Ther Umsch. 2011. PMID: 21968896 Review. German.
Cited by
-
Evaluation of the Potential Diagnostic Utility of the Determination of Selected Caspases-Markers Involved in the Regulation of Apoptosis-In Patients with Ovarian Cancer.Diagnostics (Basel). 2021 Apr 14;11(4):704. doi: 10.3390/diagnostics11040704. Diagnostics (Basel). 2021. PMID: 33919909 Free PMC article.
-
Correlation between estrogen receptor expression and prognosis in epithelial ovarian cancer: a meta-analysis.Oncotarget. 2017 May 29;8(37):62400-62413. doi: 10.18632/oncotarget.18253. eCollection 2017 Sep 22. Oncotarget. 2017. PMID: 28977954 Free PMC article.
-
A prognosis-predictive nomogram of ovarian cancer with two immune-related genes: CDC20B and PNPLA5.Oncol Lett. 2020 Nov;20(5):204. doi: 10.3892/ol.2020.12067. Epub 2020 Sep 8. Oncol Lett. 2020. PMID: 32963610 Free PMC article.
-
Potential clinical utility of liquid biopsies in ovarian cancer.Mol Cancer. 2022 May 11;21(1):114. doi: 10.1186/s12943-022-01588-8. Mol Cancer. 2022. PMID: 35545786 Free PMC article. Review.
-
UGDH promotes tumor-initiating cells and a fibroinflammatory tumor microenvironment in ovarian cancer.J Exp Clin Cancer Res. 2023 Oct 19;42(1):270. doi: 10.1186/s13046-023-02820-z. J Exp Clin Cancer Res. 2023. PMID: 37858159 Free PMC article.
References
-
- Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA: a cancer journal for clinicians. 2015;65:87–108. - PubMed
-
- Chen WQ, Zheng RS, Peter DB, Zhang SW, Zeng HG, Freddie B, Ahmedin J Yu XQ, He J. Cancer statistics in China, 2015. CA: a cancer journal for clinicians. 2015;66:115–132. - PubMed
-
- Prat J. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int J Gynecol Obste. 2014;1:1–5. - PubMed
-
- Harrison ML, Cameson C, Gore ME. Mucinous ovarian cancer. Int J Gynecol Obste. 2008;2:209–214. - PubMed
-
- Fleming GF, Seidman J, Lengyel E. Principles and Practice of Gynecologic Oncology. 6th. Philadelphia: Lippincott Williams & Wilkins; 2013.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
