

WITHDRAWN: Acupuncture for neck disorders
- PMID: 27852100
- PMCID: PMC6734124
- DOI: 10.1002/14651858.CD004870.pub5
WITHDRAWN: Acupuncture for neck disorders
Abstract
Background: Neck pain is one of the three most frequently reported complaints of the musculoskeletal system. Treatments for neck pain are varied, as are perceptions of benefit. Acupuncture has been used as an alternative to more conventional treatment for musculoskeletal pain. This review summarises the most current scientific evidence on the effectiveness of acupuncture for acute, subacute and chronic neck pain. This update replaces our 2006 Cochrane review update on this topic.
Objectives: To determine the effects of acupuncture for adults with neck pain, with focus on pain relief, disability or functional measures, patient satisfaction and global perceived effect.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, the Manual, Alternative and Natural Therapy Index System (MANTIS), the Cumulative Index to Nursing and Allied Health Literature (CINAHL) and the Index to Chiropractic Literature (ICL) from their beginning to August 2015. We searched reference lists, two trial registers and the acupuncture database Traditional Chinese Medical Literature Analysis and Retrieval System (TCMLARS) in China to 2005.
Selection criteria: We included published trials that used random assignment to intervention groups, in full text or abstract form. We excluded quasi-randomised controlled trials (RCTs).
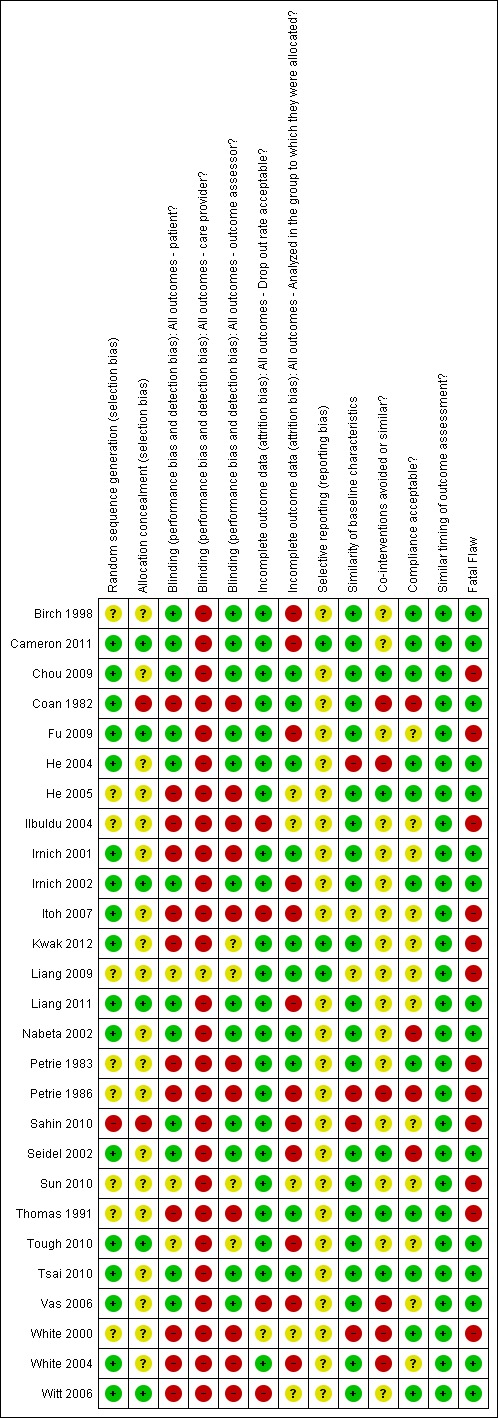
Data collection and analysis: Two review authors made independent decisions for each step of the review: article inclusion, data abstraction and assessment of quality of trial methods. We assessed study quality by using the Cochrane Back Review Group 'Risk of bias' tool. We used consensus to resolve disagreements, and when clinical heterogeneity was absent, we combined studies by using random-effects meta-analysis models.
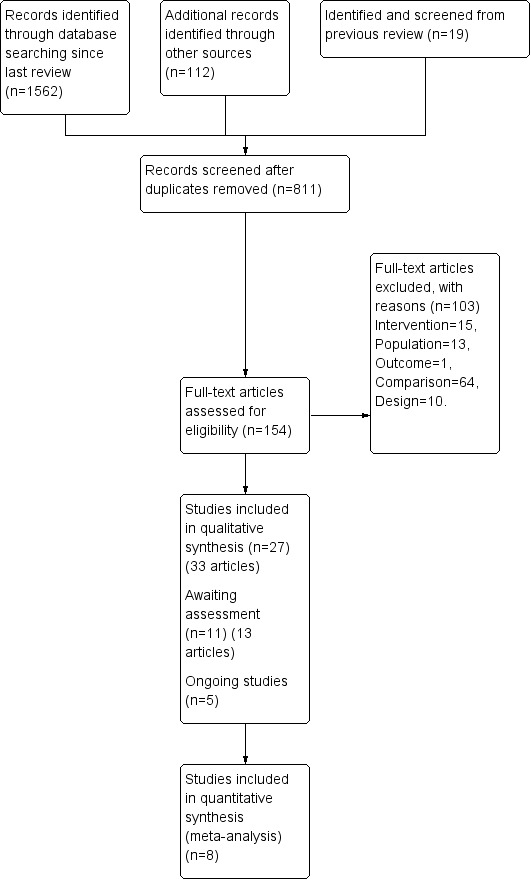
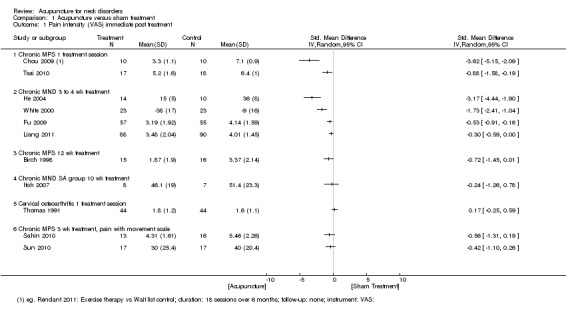
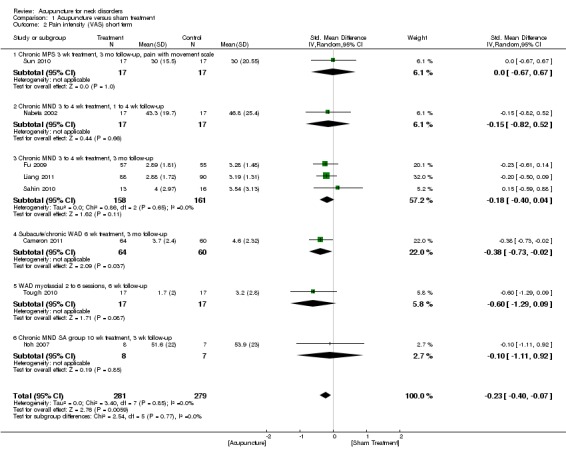
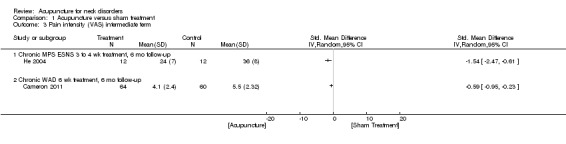
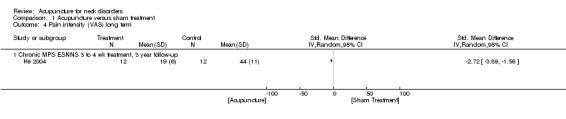
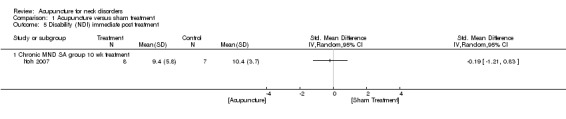
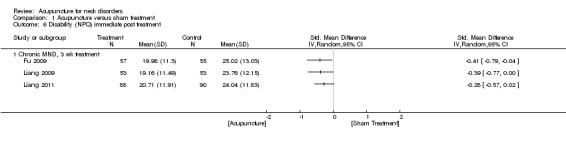
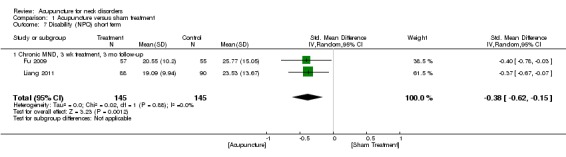
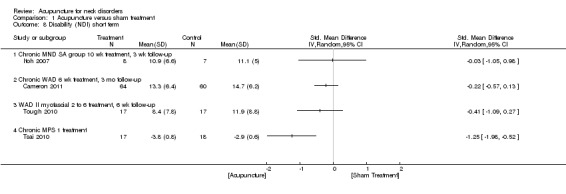
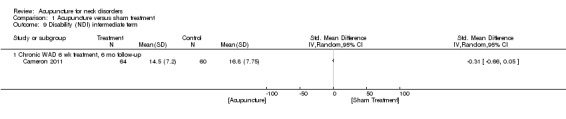
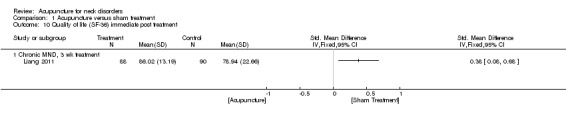
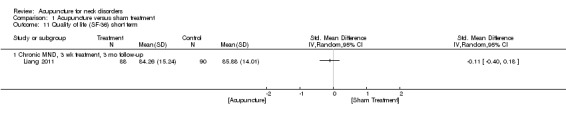
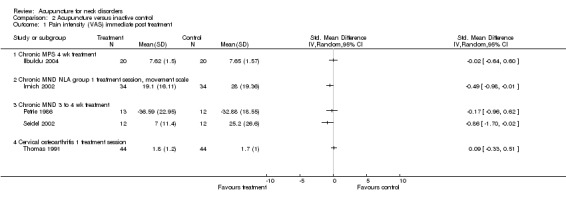
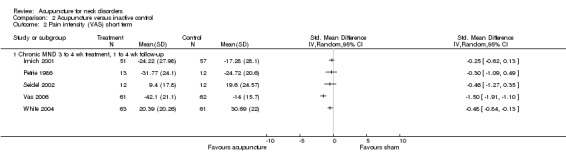
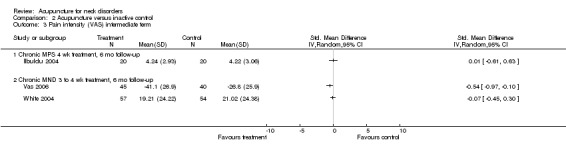
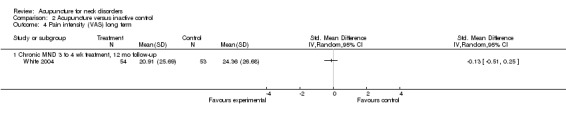
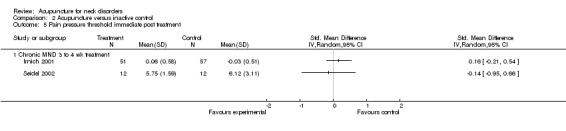
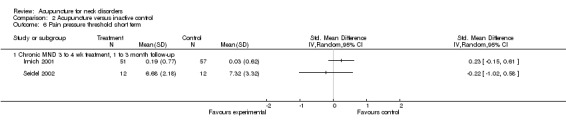
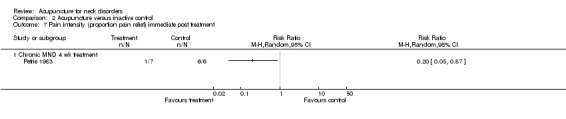
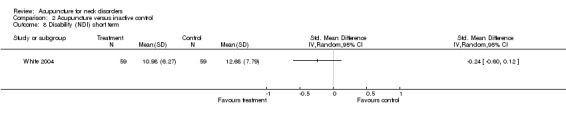
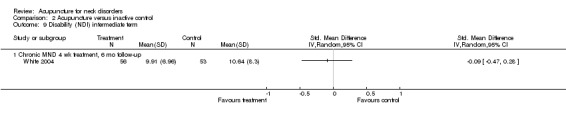
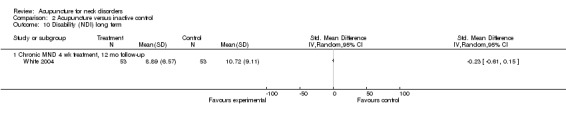
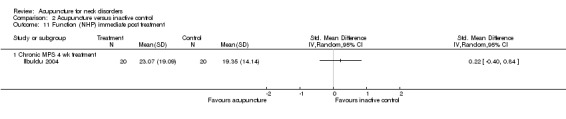
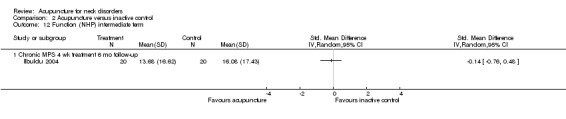
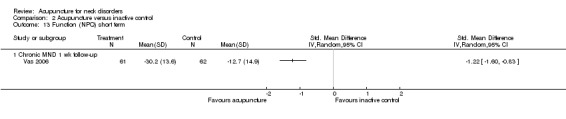
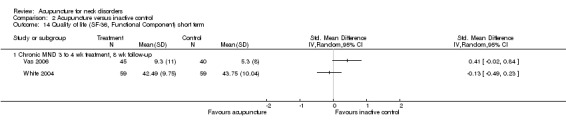
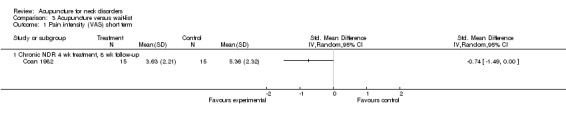
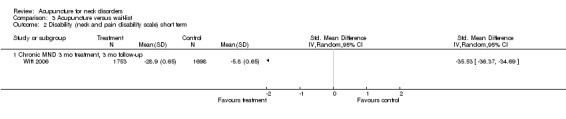
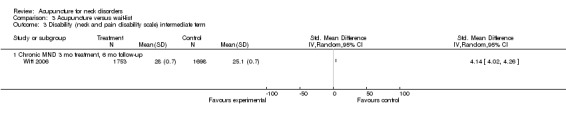
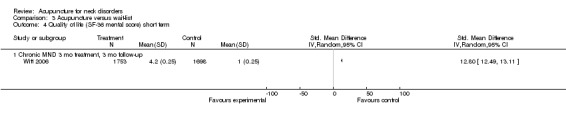
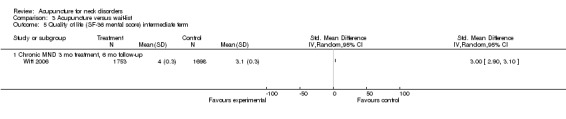
Main results: Of the 27 included studies, three represented individuals with whiplash-associated disorders (WADs) ranging from acute to chronic (205 participants), five explored chronic myofascial neck pain (186 participants), five chronic pain due to arthritic changes (542 participants), six chronic non-specific neck pain (4011 participants), two neck pain with radicular signs (43 participants) and six subacute or chronic mechanical neck pain (5111 participants).For mechanical neck pain, we found that acupuncture is beneficial at immediate-term follow-up compared with sham acupuncture for pain intensity; at short-term follow-up compared with sham or inactive treatment for pain intensity; at short-term follow-up compared with sham treatment for disability; and at short-term follow-up compared with wait-list control for pain intensity and neck disability improvement. Statistical pooling was appropriate for acupuncture compared with sham for short-term outcomes due to statistical homogeneity (P value = 0.83; I2 = 20%). Results of the meta-analysis favoured acupuncture (standardised mean difference (SMD) -0.23, 95% confidence interval (CI) -0.20 to -0.07; P value = 0.0006). This effect does not seem sustainable over the long term. Whether subsequent repeated sessions would be successful was not examined by investigators in our primary studies.Acupuncture appears to be a safe treatment modality, as adverse effects are minor. Reported adverse effects include increased pain, bruising, fainting, worsening of symptoms, local swelling and dizziness. These studies reported no life-threatening adverse effects and found that acupuncture treatments were cost-effective.Since the time of our previous review, the quality of RCTs has improved, and we have assessed many of them as having low risk of bias. However, few large trials have provided high-quality evidence.
Authors' conclusions: Moderate-quality evidence suggests that acupuncture relieves pain better than sham acupuncture, as measured at completion of treatment and at short-term follow-up, and that those who received acupuncture report less pain and disability at short-term follow-up than those on a wait-list. Moderate-quality evidence also indicates that acupuncture is more effective than inactive treatment for relieving pain at short-term follow-up.
Conflict of interest statement
D Irnich is an author of two included studies. He did not take part in data extraction.
Use of raters from diverse professional backgrounds (sports medicine physician, rheumatologist, occupational health physician, physiatrist, statistician, physiotherapist, manual therapist, chiropractor, massage therapist) should serve to limit any conflicts of interest that might have been present during the review process.
Figures
Update of
-
Acupuncture for neck disorders.Cochrane Database Syst Rev. 2016 May 4;(5):CD004870. doi: 10.1002/14651858.CD004870.pub4. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2016 Nov 17;11:CD004870. doi: 10.1002/14651858.CD004870.pub5. PMID: 27145001 Updated.
References
References to studies included in this review
-
- Birch S, Jamison R. Controlled trial of Japanese acupuncture for chronic myofascial neck pain: assessment of specific and nonspecific effects of treatment. Clinical Journal of Pain 1998;14:248‐55. [CO2002:2756] - PubMed
-
- Cameron ID, Wang E. World Congress on Neck Pain Conference Proceedings. Los Angeles, 2008.
- Cameron ID, Wang E, Sindhusake D. A randomized trial comparing acupuncture and simulated acupuncture for subacute and chronic whiplash. Spine 2011;36(26):E1659‐65. - PubMed
-
- Chou L‐W, Hsieh Y‐L, Kao M‐J, Hong C‐Z. Remote influences of acupuncture on the pain intensity and the amplitude changes of endplate noise in the myofascial trigger point of the upper trapezius muscle. Archives of Physical Medicine and Rehabilitation 2009;90:905‐12. - PubMed
-
- Coan RM, Wong G, Coan PL. The acupuncture treatment of neck pain: a randomized controlled study. American Journal of Chinese Medicine 1982;9(4):326‐32. - PubMed
-
- Fu W‐B, Liang Z‐H, Zhu X‐P, Yu P, Zhang J‐F. Analysis on the effect of acupuncture in treating cervical spondylosis with different syndrome types. Chinese Journal of Integrative Medicine 2009;15(6):426‐30. - PubMed
References to studies excluded from this review
-
- Bahadir C, Majlesi J, Unalan H. The effect of high‐power pain threshold ultrasound therapy on the electrical activity of trigger points and local twitch response on electromyography: a preliminary study. Journal of Musculoskeletal Pain 2009;17(2):162‐72. [CO2007]
-
- Calvo‐Trujillo S. Effectiveness of the Auto‐acupressure for Diminishing Neck Pain of Benign Origin, 2013. http://ClinicalTrials.gov/show/NCT01855893.
-
- Ceccherelli F, Tortora P, Nassimbeni C, Casale R, Gagliardi G, Giron G. The therapeutic efficacy of somatic acupuncture is not increased by auriculotherapy: a randomised, blind control study in cervical myofascial pain. Complementary Therapies in Medicine 2006;14:47‐52. [CO2010] - PubMed
-
- Ceccherelli F, Marino E, Caliendo A, Dezzoni R, Roveri A, Gagliardi G. 3, 5, 11 needles: looking for the perfect number of needles ‐ a randomized and controlled study. Acupuncture & Electro‐Therapeutics Research International Journal 2014;39:241‐58. - PubMed
References to studies awaiting assessment
-
- Amos Z, Yoav M, Guy A, Adi F, Yigal M, Shmuel BH. A randomised controlled trial of an integrative approach utilising acupuncture for back and neck pain in an emergency department setting. European Journal of Integrative Medicine 2012;4S:23‐4.
-
- Bar‐Haim S. Acupuncture for Back and Neck Pain in an Emergency Room Setting. clinicaltrials.gov NCT00859365.
-
- Cerezo‐Tellez E. Dry Needling of the Trapezius Muscle in Office Workers With Neck Pain. Randomised, Single Blinded Clinical Trial, 2014. http://ClinicalTrials.gov/show/NCT02219386. - PMC - PubMed
-
- Choi DY. Acupuncture for Whiplash Associated Disorder. http://ClinicalTrials.gov/show/NCT01395511.
-
- Guo Y. Efficacy of Abdominal Acupuncture for Neck Pain: A Randomized Controlled Trial. http://apps.who.int/trialsearch/AdvSearch.aspx ChiCTR‐TRC‐14004932. - PMC - PubMed
References to ongoing studies
-
- Calamita S, Biasotto‐Gonzalez D, Melo N, Meira dos Santos D, Lassa R, Mendonça F, et al. Evaluation of the immediate effect of acupuncture on pain, cervical range of motion and electromyographic activity of the upper trapezius muscle in patients with nonspecific neck pain: study protocol for a randomized controlled trial. Trials 2015;16:1. - PMC - PubMed
-
- Kim K‐H, Ryu‐J‐H, Park MR, Kim YI, Min MK, Park YM, et al. Acupuncture as analgesia for non‐emergent acute non‐specific neck pain, ankle sprain and primary headache in an emergency department setting: a protocol for a parallel group, randomised, controlled pilot trial. BMJ Open 2014;4:1‐8. - PMC - PubMed
Additional references
-
- Boutron I, Moher D, Tugwell P, Giraudeau B, Poiraudeau S, Nizard R, et al. A checklist to evaluate a report of a non pharmacological trial (CLEAR NPT) was developed using consensus. Journal of Clinical Epidemiology 2005;58:1233‐40. - PubMed
-
- Carroll LJ, Hogg‐Johnson S, Velde G, Haldeman S, Holm LW, Carragee EJ, et al. Course and prognostic factors for neck pain in the general population ‐ results of the bone and joint decade 2000‐2010 task force on neck pain and its associated disorders. Spine 2008;33(4S): S75‐82. - PubMed
-
- Chen LI, Zhang J, Li F, Qiu Y, Wang L, Li YH, et al. Endogenous anandamide and cannabinoid receptor‐2 contribute to electroacupuncture analgesia in rats. Journal of Pain 2009;10(7):732‐9. - PubMed
-
- Cicchetti DV. Assessing inter‐rater reliability for rating scales: resolving some basic issues. British Journal of Psychiatry 1976;129:452‐6. - PubMed
-
- Cohen J. Statistical Power Analysis for the Behavioural Sciences. 2nd Edition. Hilldale, NJ: Lawrence Erlbaum Associates, 1988:Lawance Erlbaum.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical