

Highly Multiplexed Proteomic Analysis of Quantiferon Supernatants To Identify Biomarkers of Latent Tuberculosis Infection
- PMID: 27852671
- PMCID: PMC5277508
- DOI: 10.1128/JCM.01646-16
Highly Multiplexed Proteomic Analysis of Quantiferon Supernatants To Identify Biomarkers of Latent Tuberculosis Infection
Erratum in
-
Correction for De Groote et al., "Highly Multiplexed Proteomic Analysis of Quantiferon Supernatants To Identify Biomarkers of Latent Tuberculosis Infection".J Clin Microbiol. 2017 May;55(5):1598. doi: 10.1128/JCM.00333-17. J Clin Microbiol. 2017. PMID: 28442616 Free PMC article. No abstract available.
Abstract
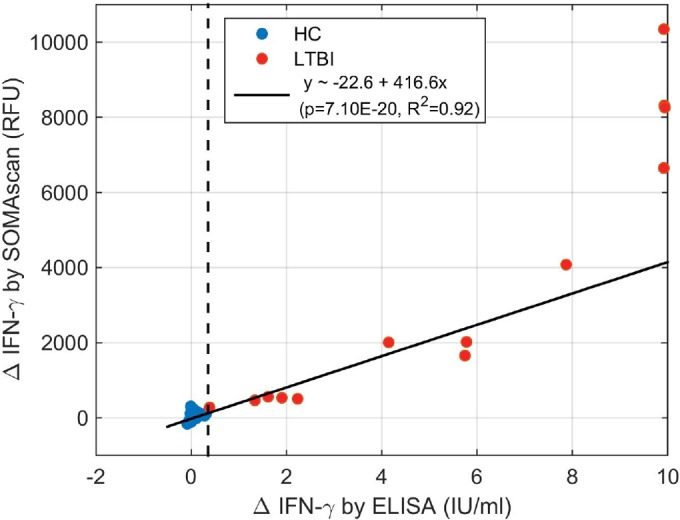
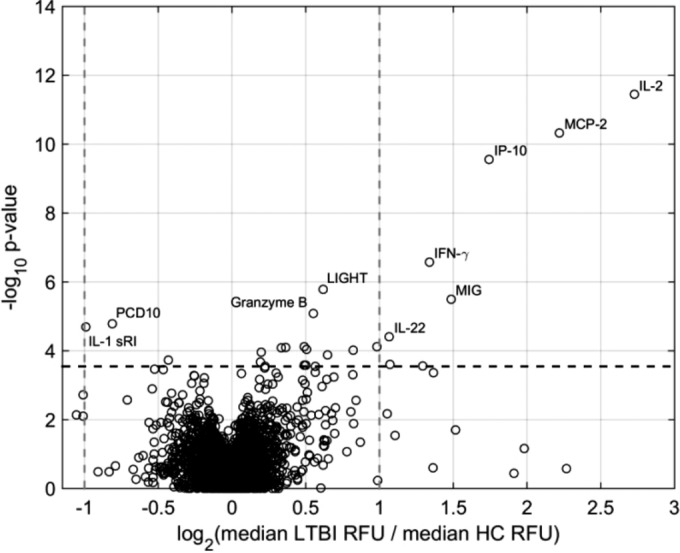
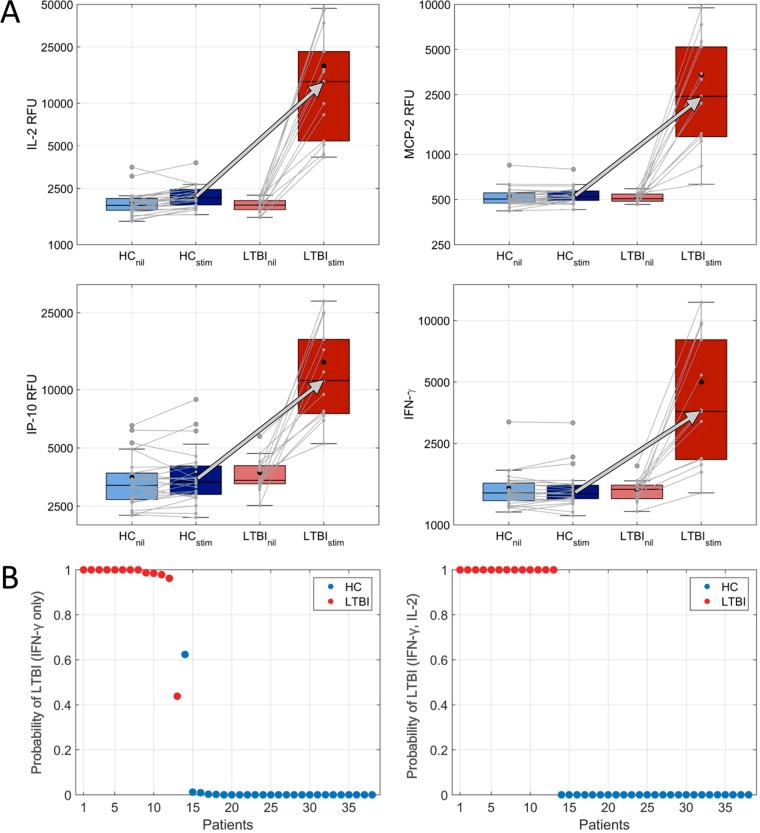
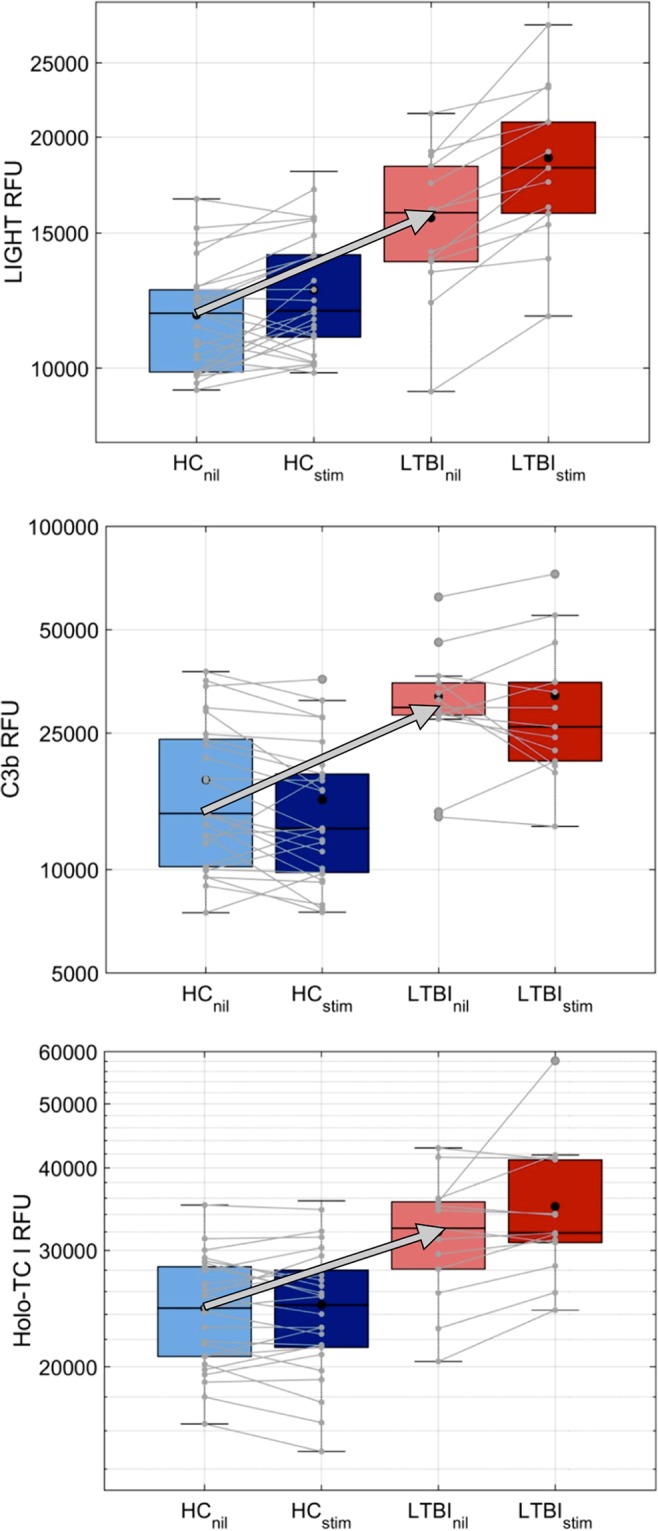
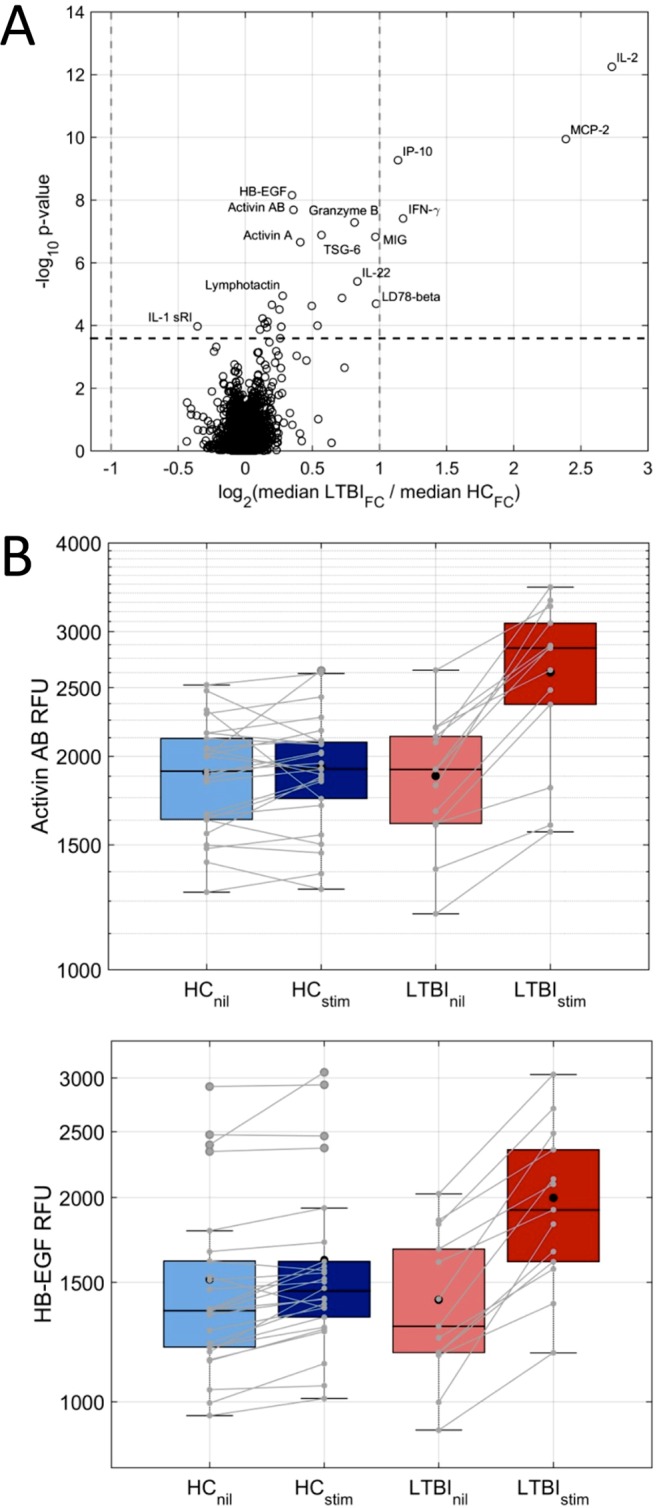
The tests for diagnosing latent tuberculosis infection (LTBI) are limited by a poor predictive value for identifying people at the highest risk for progressing to active tuberculosis (TB) and have various sensitivities and specificities in different populations. Identifying a more robust signature for LTBI is important for TB prevention and elimination. A pilot study was conducted with samples from immigrants to the United States that were screened for LTBI by the three commercially approved tests, namely, the tuberculin skin test (TST), the Quantiferon-TB Gold in-tube (QFT-GIT), and the T-SPOT.TB (T-SPOT). QFT-GIT supernatants from 13 people with concordant positive results and 26 people with concordant negative results were analyzed via the highly multiplexed SOMAscan proteomic assay. The proteins in the stimulated supernatants that distinguished LTBI from controls included interleukin-2 (IL-2), monocyte chemotactic protein 2 (MCP-2), interferon gamma inducible protein-10 (IP-10), interferon gamma (IFN-γ), tumor necrosis factor superfamily member 14 (TNFSF14, also known as LIGHT), monokine induced by gamma interferon (MIG), and granzyme B (P <0.00001). In addition, antigen stimulation increased the expression of heparin-binding EGF-like growth factor (HB-EGF) and activin AB in LTBI samples. In nil tubes, LIGHT was the most significant marker (P <0.0001) and was elevated in LTBI subjects. Other prominent markers in nonstimulated QFT-GIT supernatants were the complement-3 components C3b, iC3b, and C3d, which were upregulated in LTBI and markedly decreased upon stimulation. We found known and novel proteins that warrant further studies for developing improved tests for LTBI, for predicting progression to active disease, and for discriminating LTBI from active TB.
Keywords: biomarkers; diagnosis; immunity; latent infection; proteomics; tuberculosis.
Copyright © 2017 De Groote et al.
Figures
References
-
- World Health Organization. 2016. Global tuberculosis report. World Health Organization, Geneva, Switzerland: http://www.who.int/tb/publications/global_report/en/.
-
- World Health Organization. 2015. Guidelines on the management of latent tuberculosis infection. World Health Organization, Geneva, Switzerland: www.who.int/tb/publications/ltbi_document_page/en/. - PubMed
-
- Dorman SE, Belknap R, Graviss EA, Reves R, Schluger N, Weinfurter P, Wang Y, Cronin W, Hirsch-Moverman Y, Teeter LD, Parker M, Garrett DO, Daley CL. 2014. Interferon gamma release assays and tuberculin skin testing for diagnosis of latent tuberculosis infection in healthcare workers in the United States. Am J Respir Crit Care Med 189:77–87. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
