

Validation of diagnostic characteristics of needle based confocal laser endomicroscopy in differentiation of pancreatic cystic lesions
- PMID: 27853737
- PMCID: PMC5110338
- DOI: 10.1055/s-0042-116491
Validation of diagnostic characteristics of needle based confocal laser endomicroscopy in differentiation of pancreatic cystic lesions
Abstract
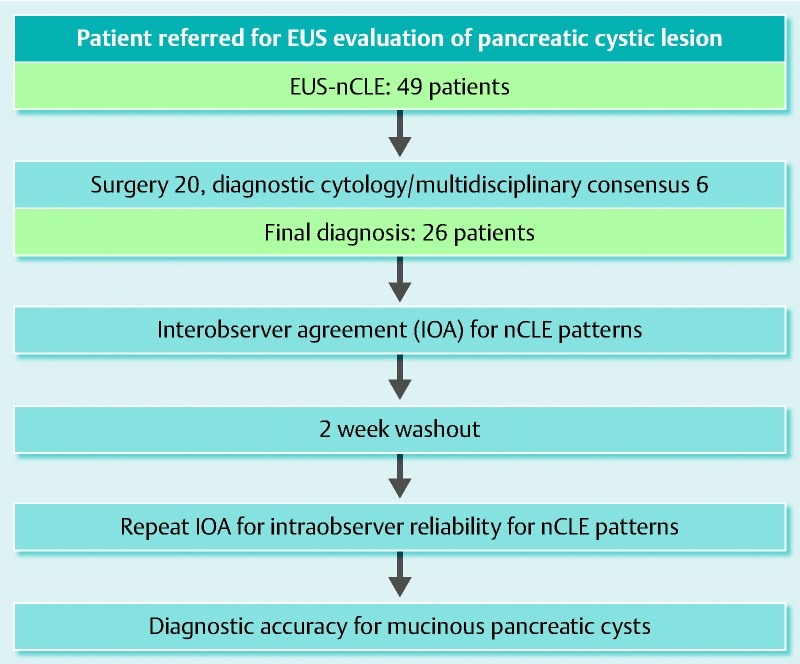
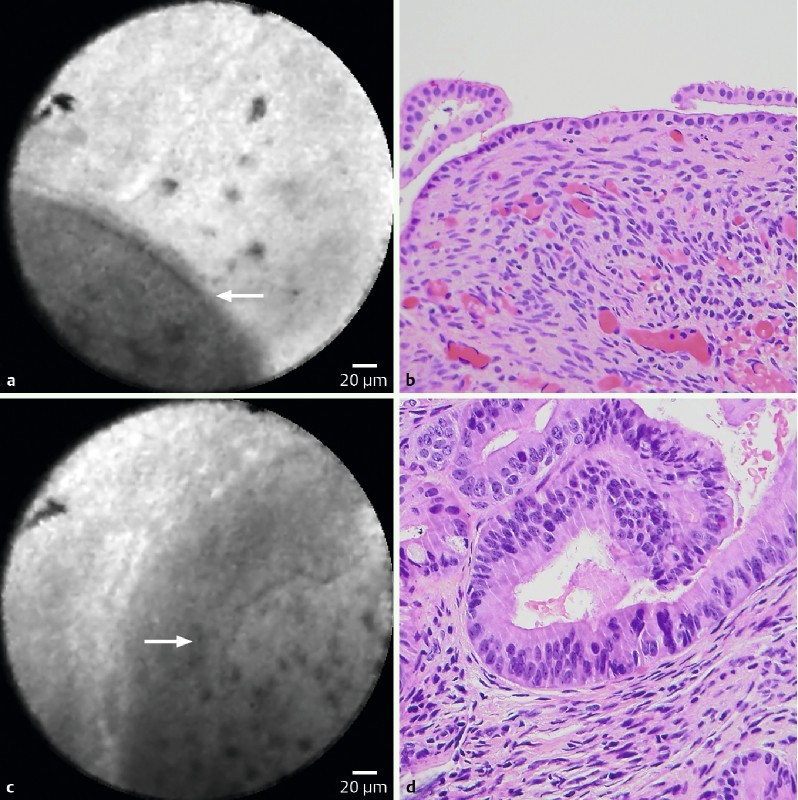
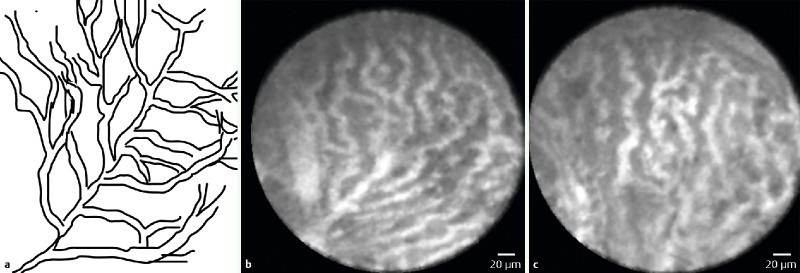
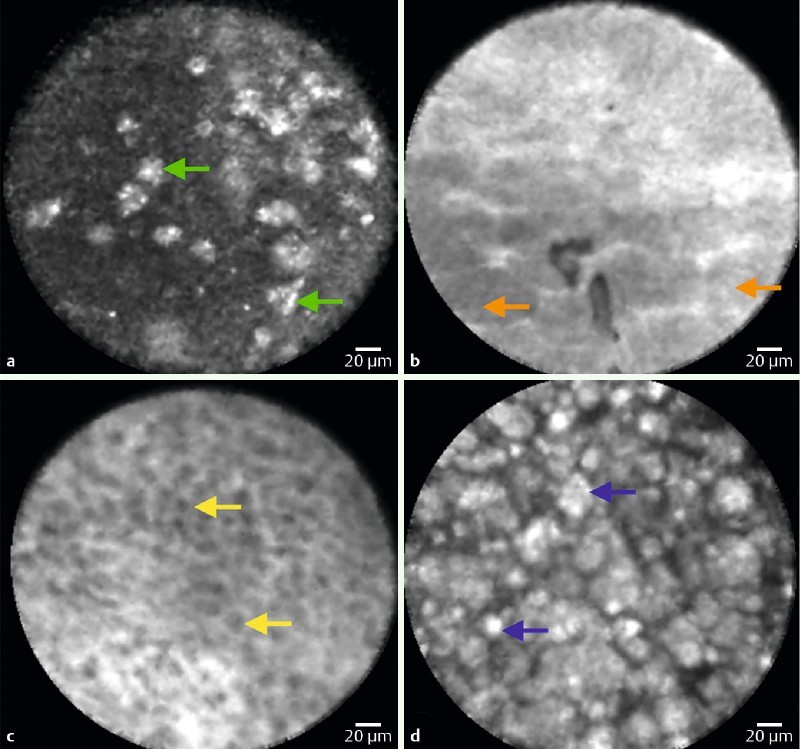
Background and aims: Endoscopic ultrasound (EUS)-guided needle-based Confocal Laser Endomicroscopy (nCLE) characteristics of pancreatic cystic lesions (PCLs) have been identified in studies where the gold standard surgical histopathology was available in a minority of patients. There are diverging reports of interobserver agreement (IOA) and paucity of intraobserver reliability (IOR). Thus, we sought to validate current EUS-nCLE criteria of PCLs in a larger consecutive series of surgical patients. Methods: A retrospective analysis of patients who underwent EUS-nCLE at a single center was performed. For calculation of IOA (Fleiss' kappa) and IOR (Cohen's kappa), blinded nCLE-naïve observers (n = 6) reviewed nCLE videos of PCLs in two phases separated by a 2-week washout period. Results: EUS-nCLE was performed in 49 subjects, and a definitive diagnosis was available in 26 patients. The overall sensitivity, specificity, and accuracy for diagnosing a mucinous PCL were 94 %, 82 %, and 89 %, respectively. The IOA for differentiating mucinous vs. non-mucinous PCL was "substantial" (κ = 0.67, 95 %CI 0.57, 0.77). The mean (± standard deviation) IOR was "substantial" (κ = 0.78 ± 0.13) for diagnosing mucinous PCLs. Both the IOAs and mean IORs were "substantial" for detection of known nCLE image patterns of papillae/epithelial bands of mucinous PCLs (IOA κ = 0.63; IOR κ = 0.76 ± 0.11), bright particles on a dark background of pseudocysts (IOA κ = 0.71; IOR κ = 0.78 ± 0.12), and fern-pattern or superficial vascular network of serous cystadenomas (IOA κ = 0.62; IOR κ = 0.68 ± 0.20). Three (6.1 % of 49) patients developed post-fine needle aspiration (FNA) pancreatitis. Conclusion: Characteristic EUS-nCLE patterns can be consistently identified and improve the diagnostic accuracy of PCLs. These results support further investigations to optimize EUS-nCLE while minimizing adverse events.
Study registration: NCT02516488.
Conflict of interest statement
Figures

References
-
- de Jong K, Nio C Y, Hermans J J. et al.High prevalence of pancreatic cysts detected by screening magnetic resonance imaging examinations. Clin Gastroenterol Hepatol. 2010;8:806–811. - PubMed
-
- Tanaka M, Fernandez-del Castillo C, Adsay V. et al.International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology. 2012;12:183–197. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical