

Acute Kidney Injury as a Risk Factor for Delirium and Coma during Critical Illness
- PMID: 27854517
- PMCID: PMC5476907
- DOI: 10.1164/rccm.201603-0476OC
Acute Kidney Injury as a Risk Factor for Delirium and Coma during Critical Illness
Abstract
Rationale: Acute kidney injury may contribute to distant organ dysfunction. Few studies have examined kidney injury as a risk factor for delirium and coma.
Objectives: To examine whether acute kidney injury is associated with delirium and coma in critically ill adults.
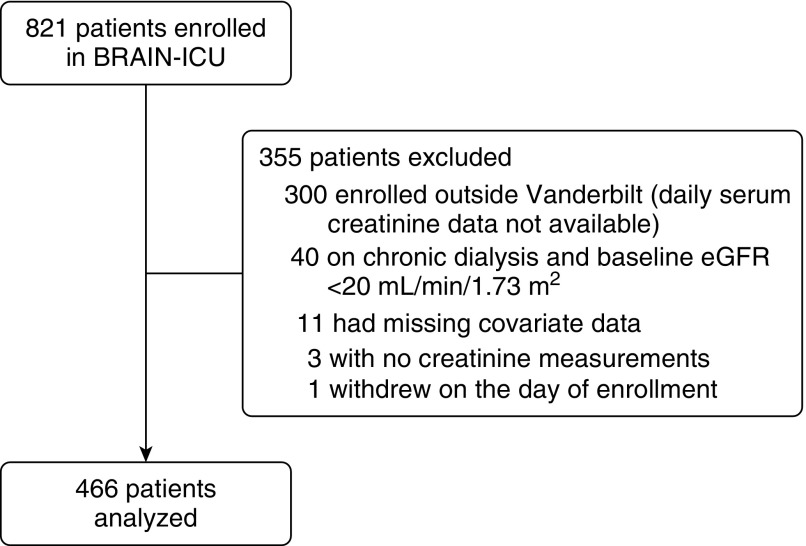
Methods: In a prospective cohort study of intensive care unit patients with respiratory failure and/or shock, we examined the association between acute kidney injury and daily mental status using multinomial transition models adjusting for demographics, nonrenal organ failure, sepsis, prior mental status, and sedative exposure. Acute kidney injury was characterized daily using the difference between baseline and peak serum creatinine and staged according to Kidney Disease Improving Global Outcomes criteria. Mental status (normal vs. delirium vs. coma) was assessed daily with the Confusion Assessment Method for the ICU and Richmond Agitation-Sedation Scale.
Measurements and main results: Among 466 patients, stage 2 acute kidney injury was a risk factor for delirium (odds ratio [OR], 1.55; 95% confidence interval [CI], 1.07-2.26) and coma (OR, 2.04; 95% CI, 1.25-3.34) as was stage 3 injury (OR for delirium, 2.56; 95% CI, 1.57-4.16) (OR for coma, 3.34; 95% CI, 1.85-6.03). Daily peak serum creatinine (adjusted for baseline) values were also associated with delirium (OR, 1.35; 95% CI, 1.18-1.55) and coma (OR, 1.44; 95% CI, 1.20-1.74). Renal replacement therapy modified the association between stage 3 acute kidney injury and daily peak serum creatinine and both delirium and coma.
Conclusions: Acute kidney injury is a risk factor for delirium and coma during critical illness.
Keywords: acute kidney injury; coma; critical illness; delirium.
Figures


Comment in
-
Kidney and Brain, an Unbroken Chain.Am J Respir Crit Care Med. 2017 Jun 15;195(12):1546-1548. doi: 10.1164/rccm.201611-2371ED. Am J Respir Crit Care Med. 2017. PMID: 28617085 Free PMC article. No abstract available.
References
-
- Hoste EA, Bagshaw SM, Bellomo R, Cely CM, Colman R, Cruz DN, Edipidis K, Forni LG, Gomersall CD, Govil D, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41:1411–1423. - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, et al. Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. - PubMed
-
- Ali T, Khan I, Simpson W, Prescott G, Townend J, Smith W, Macleod A. Incidence and outcomes in acute kidney injury: a comprehensive population-based study. J Am Soc Nephrol. 2007;18:1292–1298. - PubMed
-
- Amdur RL, Chawla LS, Amodeo S, Kimmel PL, Palant CE. Outcomes following diagnosis of acute renal failure in U.S. veterans: focus on acute tubular necrosis. Kidney Int. 2009;76:1089–1097. - PubMed
-
- Amin AP, Salisbury AC, McCullough PA, Gosch K, Spertus JA, Venkitachalam L, Stolker JM, Parikh CR, Masoudi FA, Jones PG, et al. Trends in the incidence of acute kidney injury in patients hospitalized with acute myocardial infarction. Arch Intern Med. 2012;172:246–253. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
