

The Influence of Cyclic Hormonal Contraception on Expression of Premenstrual Syndrome
- PMID: 27854559
- PMCID: PMC5397197
- DOI: 10.1089/jwh.2016.5941
The Influence of Cyclic Hormonal Contraception on Expression of Premenstrual Syndrome
Abstract
Background: Some women who use cyclic hormonal contraception (CHC) suffer from premenstrual symptoms; whether their symptoms differ from women who do not use CHC is not clear.
Objective: To compare women who use or do not use CHC on perimenstrual symptom timing and change severity.
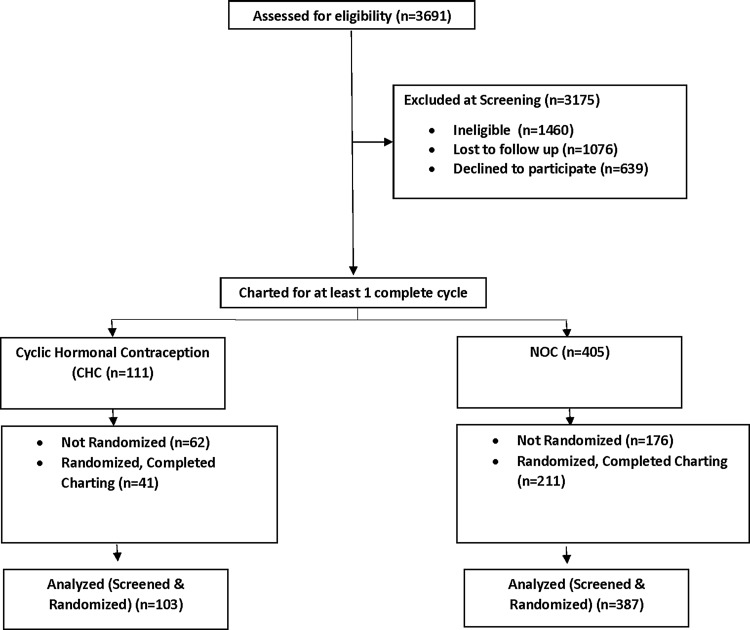
Study design: We analyzed daily symptom ratings from women who requested participation in (Screened Cohort: 103 used CHC and 387 did not) or were randomized in (Randomized Cohort: 41 used CHC and 211 did not) a clinical trial for premenstrual syndrome. We used effect sizes to compute and compare change scores between cycle phases in four partially overlapping perimenstrual windows defined relative to day 1 of menses [(-6, -1), (-5, 1), (-4, 2), (-3, 3)]. Differences in magnitude of change and timing were estimated using linear mixed-effects models.
Results: Both cohorts showed a significant two-way interaction between CHC use and symptom change scores (p < 0.01) and a significant main effect of perimenstrual window (p < 0.0001). Overall menstrual cycle symptom change was greater for the nonhormonal contraception versus hormonal contraception group. In the Screened Cohort, change scores were greater in the nonhormonal group specifically for depression (p = 0.04); anger or irritability (p < 0.01); and physical symptoms (p < 0.01). Mean change scores increased as the window shifted forward toward menses for both cohorts with the largest effect size and greatest group difference for (-4, 2) interval.
Conclusions: CHC slightly attenuates menstrual cycle symptom change. The (-4, 2) perimenstrual interval shows the largest change compared with postmenses.
Keywords: contraception; menstrual cycle; mental health.
Conflict of interest statement
Dr. Yonkers discloses royalties from UpToDate and consulting to Pontifax; Dr. Gueorguieva discloses consulting fees from Palo Alto Health Sciences and Mathematica Policy Research; Dr. Kornstein discloses research support from Palatin Technologies, Takeda, Allergan, Forest, Roche, and Pfizer; consulting or participation in advisory boards for Palatin Technologies, Takeda, Allergan, Forest, Naurex, Pfizer, Lilly, Shire, and Sunovion; and royalties from Guilford Press; and Dr. Altemus and Ms. Cameron have no conflicts of interest.
References
-
- ACOG. ACOG issues guidelines on diagnosis and treatment of PMS. 2003. www.acog.org/patients/FAQs/premenstrual-syndrome-PMS Accessed May1, 2015
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th ed. Washington, DC: American Psychiatric Association; 2013
-
- Hurt SW, Schnurr PP, Severino SK, et al. Late luteal phase dysphoric disorder in 670 women evaluated for premenstrual complaints. Am J Psychiatry 1992;149:525–530 - PubMed
-
- Hartlage SA, Arduino KE. Toward the content validity of premenstrual dysphoric disorder: Do anger and irritability more than depressed mood represent treatment seekers experiences? Psychol Rep 2002;90:189–202 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
