

Low Caspofungin Exposure in Patients in Intensive Care Units
- PMID: 27855112
- PMCID: PMC5278683
- DOI: 10.1128/AAC.01582-16
Low Caspofungin Exposure in Patients in Intensive Care Units
Abstract
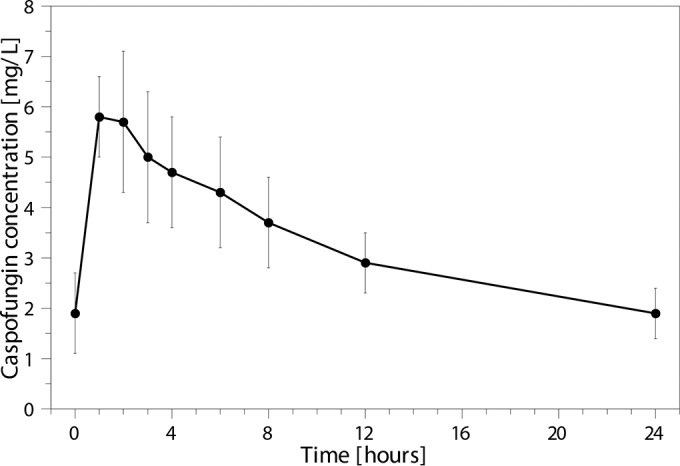
In critically ill patients, drug exposure may be influenced by altered drug distribution and clearance. Earlier studies showed that the variability in caspofungin exposure was high in intensive care unit (ICU) patients. The primary objective of this study was to determine if the standard dose of caspofungin resulted in adequate exposure in critically ill patients. A multicenter prospective study in ICU patients with (suspected) invasive candidiasis was conducted in the Netherlands from November 2013 to October 2015. Patients received standard caspofungin treatment, and the exposure was determined on day 3 of treatment. An area under the concentration-time curve from 0 to 24 h (AUC0-24) of 98 mg · h/liter was considered adequate exposure. In case of low exposure (i.e., <79 mg · h/liter, a ≥20% lower AUC0-24), the caspofungin dose was increased and the exposure reevaluated. Twenty patients were included in the study, of whom 5 had a positive blood culture. The median caspofungin AUC0-24 at day 3 was 78 mg · h/liter (interquartile range [IQR], 69 to 97 mg · h/liter). A low AUC0-24 (<79 mg · h/liter) was seen in 10 patients. The AUC0-24 was significantly and positively correlated with the caspofungin dose in mg/kg/day (P = 0.011). The median AUC0-24 with a caspofungin dose of 1 mg/kg was estimated using a pharmacokinetic model and was 114.9 mg · h/liter (IQR, 103.2 to 143.5 mg · h/liter). In conclusion, the caspofungin exposure in ICU patients in this study was low compared with that in healthy volunteers and other (non)critically ill patients, most likely due to a larger volume of distribution. A weight-based dose regimen is probably more suitable for patients with substantially altered drug distribution. (This study has been registered at ClinicalTrials.gov under registration no. NCT01994096.).
Keywords: antifungal therapy; intensive care; pharmacokinetics; therapeutic drug monitoring.
Copyright © 2017 American Society for Microbiology.
Figures
References
-
- Blumberg HM, Jarvis WR, Soucie JM, Edwards JE, Patterson JE, Pfaller MA, Rangel Frausto MS, Rinaldi MG, Saiman L, Wiblin RT, Wenzel RP. 2001. Risk factors for candidal bloodstream infections in surgical intensive care unit patients: the NEMIS prospective multicenter study. Clin Infect Dis 33:177–186. doi:10.1086/321811. - DOI - PubMed
-
- Magill SS, Edwards JR, Bamberg W, Beldavs ZG, Dumyati G, Kainer MA, Lynfield R, Maloney M, McAllister-Hollod L, Nadle J, Ray SM, Thompson DL, Wilson LE, Fridkin SK. 2014. Multistate point-prevalence survey of health care-associated infections. N Engl J Med 370:1198–1208. doi:10.1056/NEJMoa1306801. - DOI - PMC - PubMed
-
- Pfaller M, Neofytos D, Diekema D, Azie N, Meier-Kriesche HU, Quan SP, Horn D. 2012. Epidemiology and outcomes of candidemia in 3648 patients: data from the Prospective Antifungal Therapy (PATH Alliance®) registry, 2004-2008. Diagn Microbiol Infect Dis 74:323–323. doi:10.1016/j.diagmicrobio.2012.10.003. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
