

Modelling the effect of short-course multidrug-resistant tuberculosis treatment in Karakalpakstan, Uzbekistan
- PMID: 27855693
- PMCID: PMC5114735
- DOI: 10.1186/s12916-016-0723-2
Modelling the effect of short-course multidrug-resistant tuberculosis treatment in Karakalpakstan, Uzbekistan
Abstract
Background: Multidrug-resistant tuberculosis (MDR-TB) is a major threat to global TB control. MDR-TB treatment regimens typically have a high pill burden, last 20 months or more and often lead to unsatisfactory outcomes. A 9-11 month regimen with seven antibiotics has shown high success rates among selected MDR-TB patients in different settings and is conditionally recommended by the World Health Organization.
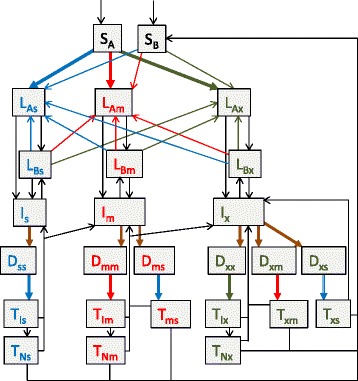
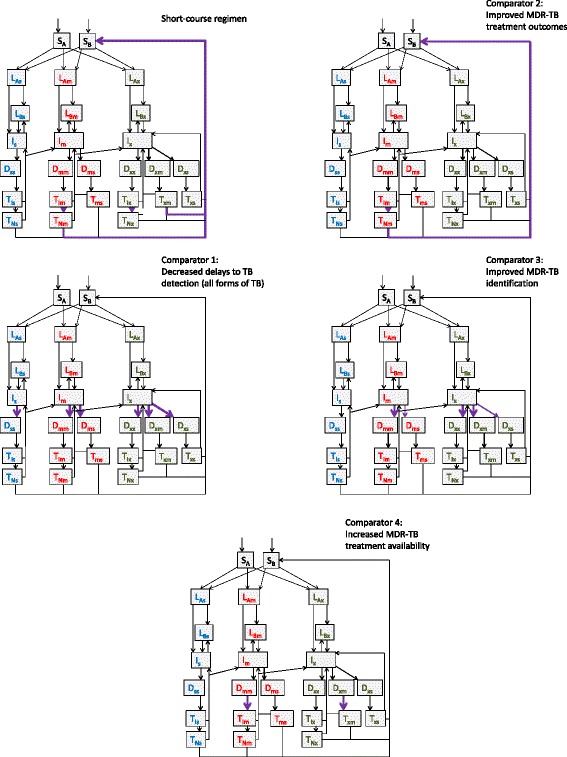
Methods: We construct a transmission-dynamic model of TB to estimate the likely impact of a shorter MDR-TB regimen when applied in a low HIV prevalence region of Uzbekistan (Karakalpakstan) with high rates of drug resistance, good access to diagnostics and a well-established community-based MDR-TB treatment programme providing treatment to around 400 patients. The model incorporates acquisition of additional drug resistance and incorrect regimen assignment. It is calibrated to local epidemiology and used to compare the impact of shorter treatment against four alternative programmatic interventions.
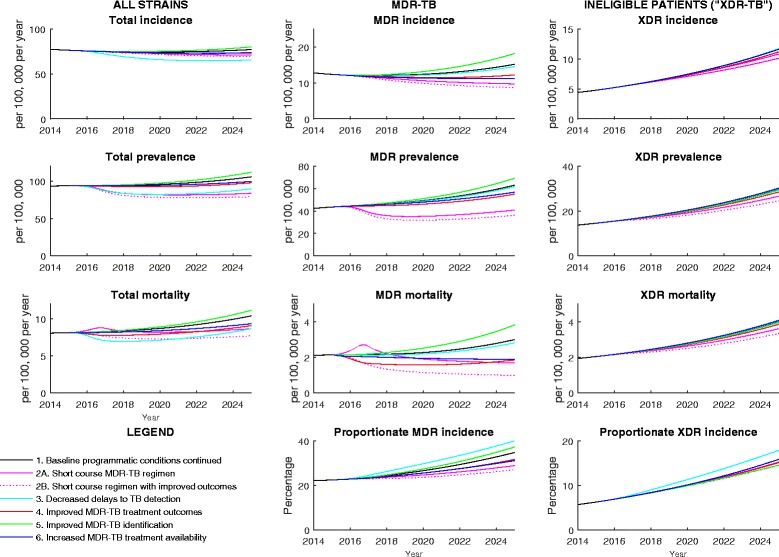
Results: Based on empirical outcomes among MDR-TB patients and assuming no improvement in treatment success rates, the shorter regimen reduced MDR-TB incidence from 15.2 to 9.7 cases per 100,000 population per year and MDR-TB mortality from 3.0 to 1.7 deaths per 100,000 per year, achieving comparable or greater gains than the alternative interventions. No significant increase in the burden of higher levels of resistance was predicted. Effects are probably conservative given that the regimen is likely to improve success rates.
Conclusions: In addition to benefits to individual patients, we find that shorter MDR-TB treatment regimens also have the potential to reduce transmission of resistant strains. These findings are in the epidemiological setting of treatment availability being an important bottleneck due to high numbers of patients being eligible for treatment, and may differ in other contexts. The high proportion of MDR-TB with additional antibiotic resistance simulated was not exacerbated by programmatic responses and greater gains may be possible in contexts where the regimen is more widely applicable.
Keywords: Epidemiology; Extensively drug-resistant tuberculosis; Modelling; Multidrug-resistant tuberculosis; Public health; Treatment; Tuberculosis; Uzbekistan.
Figures
References
-
- World Health Organization. Sixty-Second World Health Assembly. 2009. http://apps.who.int/gb/ebwha/pdf_files/WHA62-REC1/WHA62_REC1-en.pdf. Accessed 7 Mar 2016.
-
- World Health Organization. Global Tuberculosis Report 2015. 2015. http://apps.who.int/iris/bitstream/10665/191102/1/9789241565059_eng.pdf?.... Accessed 12 Nov 2015.
-
- World Health Organization. Uzbekistan, Tuberculosis Profile. 2015. https://extranet.who.int/sree/Reports?op=Replet&name=%2FWHO_HQ_Reports%2.... Accessed 18 Jan 2016.
-
- Ulmasova DJ, Uzakova G, Tillyashayhov MN, et al. Multidrug-resistant tuberculosis in Uzbekistan: results of a nationwide survey, 2010 to 2011. Euro Surveill. 2013;18(42). pii: 20609. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
