

Severe hemolytic disease of the premature newborn due to RH1 incompatibility: a case report
- PMID: 27857529
- PMCID: PMC5111500
- DOI: 10.15386/cjmed-578
Severe hemolytic disease of the premature newborn due to RH1 incompatibility: a case report
Abstract
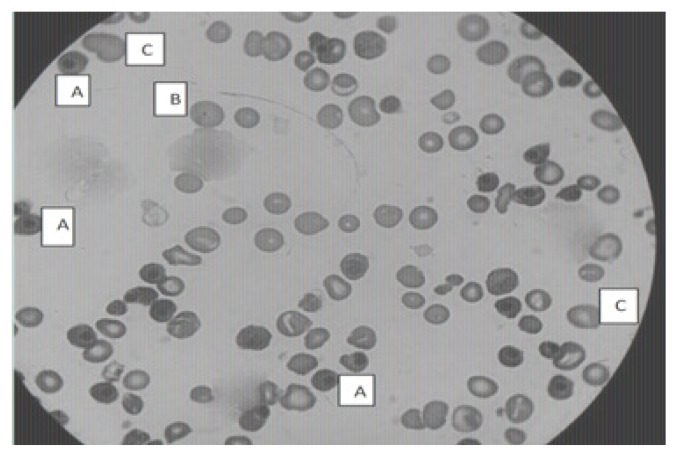
We report a case of dramatic outcome of severe hemolytic disease in a newborn due to RH1 incompatibility. A newborn with A RH1 blood group was admitted in the Mohammed V Military Teaching Hospital for the problem of hydrops fetalis associated with RH1 incompatibility. The blood group of his mother, aged 31, was AB RH1-negative and that of his 37 year old father was A RH1. The mother had a history of 4 term deliveries, 3 abortions, and 1 living child. There was no prevention by anti-D immunoglobulin postpartum. The mother's irregular agglutinin test was positive and the pregnancy was poorly monitored. The laboratory tests of the newborn showed a high total serum bilirubin level (30 mg/L) and macrocytic regenerative anemia (Hemoglobin=4 g/dL, mean corpuscular volume = 183 fL, reticulocytes count =176600/m3). The blood smear showed 1256 erythroblasts per 100 leukocytes, Howell-Jolly bodies and many macrocytes. The direct antiglobulin test was positive. He was transfused with red blood cell concentrates and treated with conventional phototherapy. The evolution was unfavourable; he died three days after the death of his mother. The monitoring of these high-risk pregnancies requires specialized centers and a close collaboration between the gynaecologist and the blood transfusion specialist to strengthen the prevention, as well as clinico-biological monitoring in patients with a history of RH1 fetomaternal alloimunization.
Keywords: Hemolytic disease of the newborn; RH1; alloimmunization; prevention.
Figures
Similar articles
-
Hemolytic disease of the fetus and newborn with late-onset anemia due to anti-M: a case report and review of the Japanese literature.Transfus Med Rev. 2014 Jan;28(1):1-6. doi: 10.1016/j.tmrv.2013.10.002. Epub 2013 Oct 19. Transfus Med Rev. 2014. PMID: 24262303 Review.
-
Hemolytic disease of the newborn caused by irregular blood subgroup (Kell, C, c, E, and e) incompatibilities: report of 106 cases at a tertiary-care centre.Am J Perinatol. 2012 Jun;29(6):449-54. doi: 10.1055/s-0032-1304826. Epub 2012 Mar 7. Am J Perinatol. 2012. PMID: 22399212
-
An early (sixth-hour) serum bilirubin measurement is useful in predicting the development of significant hyperbilirubinemia and severe ABO hemolytic disease in a selective high-risk population of newborns with ABO incompatibility.Pediatrics. 2002 Apr;109(4):e53. doi: 10.1542/peds.109.4.e53. Pediatrics. 2002. PMID: 11927726 Clinical Trial.
-
Maternal ABO-mismatched blood for intrauterine transfusion of severe hemolytic disease of the newborn due to anti-Rh17.Transfusion. 2004 Sep;44(9):1357-60. doi: 10.1111/j.1537-2995.2004.04082.x. Transfusion. 2004. PMID: 15318861
-
Anemic Disease of the Newborn With Little Increase in Hemolysis and Erythropoiesis Due to Maternal Anti-Jra: A Case Study and Review of the Literature.Transfus Med Rev. 2019 Jul;33(3):183-188. doi: 10.1016/j.tmrv.2019.03.002. Epub 2019 Apr 26. Transfus Med Rev. 2019. PMID: 31227265 Review.
Cited by
-
Unexpected discovery of multiple myeloma following cardiomyopathy.Clin Case Rep. 2017 Nov 28;6(1):86-90. doi: 10.1002/ccr3.1297. eCollection 2018 Jan. Clin Case Rep. 2017. PMID: 29375844 Free PMC article.
References
-
- Tasseau A, Rigourd V. Anémie néonatale précoce: orientation diagnostique. Journal de pédiatrie et de puériculture. 2004;17:198–203.
-
- Branger B, Winer N. Épidémiologie de l’allo-immunisation anti-D pendant la grossesse. J Gynecol Obstet Biol Reprod. 2006;35(1 Suppl):1S87–1S92. - PubMed
-
- CNGOF. Prévention de l’allo-immunisation Rhésus D foetomaternelle. Recommandations pour la pratique clinique. J Gynecol Obstet Biol Reprod. 2006;35:1S131–IS135.
-
- Mannessier L. La surveillance immunohématologique de la femme enceinte et la nouvelle politique de prévention de l’allo-immunisation anti-RH1. Transfus Clin Biol. 2007;14(1):112–119. - PubMed
-
- Rigal D, Meyer F. Anémies hémolytiques auto-immunes : diagnostic biologique et nouvelles approches thérapeutiques. Transfus Clin Biol. 2011;18:277–285. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources