

The feasibility of two new anthropometric indices to identify hypertension in rural China: A cross-sectional study
- PMID: 27858905
- PMCID: PMC5591153
- DOI: 10.1097/MD.0000000000005301
The feasibility of two new anthropometric indices to identify hypertension in rural China: A cross-sectional study
Abstract
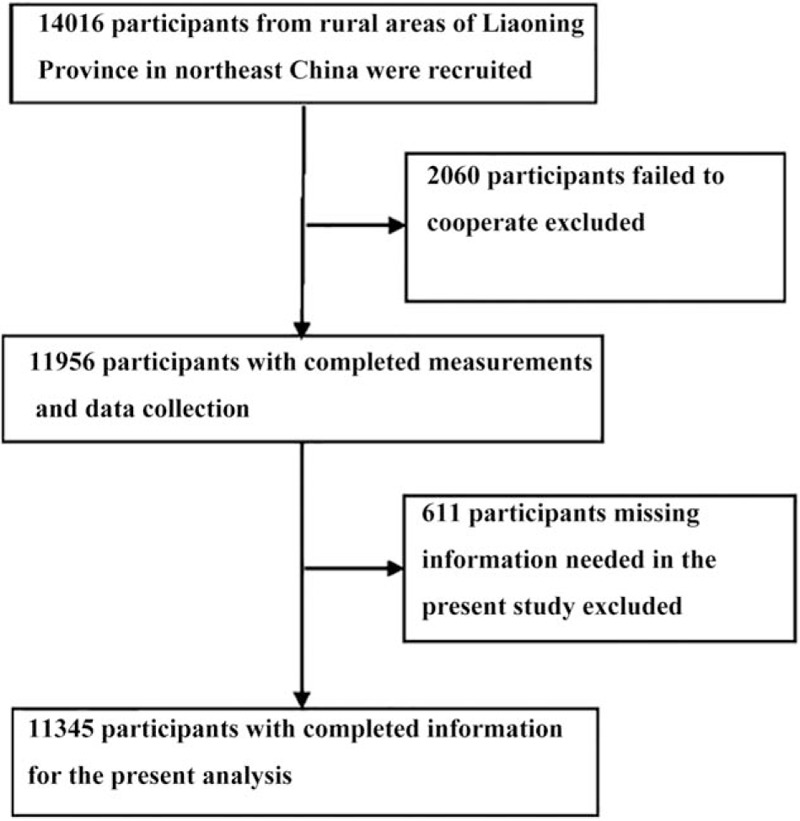
Recently, 2 new anthropometric indices, the A Body Shape Index (ABSI) and Body Roundness Index (BRI), have been developed. Our study was to compare the associations between different anthropometric indices, including ABSI, BRI, body mass index (BMI), waist circumference (WC) and waist-to-hip ratio (WHR), and hypertension in a rural population of northeast China.This cross-sectional study was conducted in the rural areas of northeast China from January 2012 to August 2013 using a multistage, stratified random cluster-sampling scheme. All eligible permanent residents aged ≥35 years (a total of 14,016 individuals) in each village were invited to participate in the study. A final sample size of 11,345 (5253 males and 6092 females) were included in this study.All the 5 anthropometric measures were positively correlated with hypertension. The prevalence of hypertension increased across quartiles for ABSI, BMI, BRI, WC, and WHR. Multivariable logistic regression analysis of the presence of hypertension for the highest quartile versus the lowest quartile of each anthropometric measure, showed that BRI had the largest values of ORs (OR: 3.49, 95% CI: 2.86-4.21 in men; OR: 3.06, 95% CI: 2.56-3.67 in women) and ABSI had the smallest ORs (OR: 1.30, 95% CI: 1.06-1.58 in men; OR: 1.19, 95% CI: 1.04-1.34 in women). BRI had the highest AROCs for hypertension (AROC: 0.65, 95% CI: 0.64-0.67 for men and AROC: 0.68, 95% CI: 0.67-0.70 for women), while ABSI had the lowest AROCs for hypertension (AROC: 0.60, 95% CI: 0.58-0.61 for men and AROC: 0.59, 95% CI: 0.58-0.61 for women).Our results showed that ABSI, BMI, BRI, WC, and WHR were all associated with hypertension. ABSI showed the weakest association with hypertension, while BRI showed potential for use as an alternative obesity measure in assessment of hypertension.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
References
-
- Poirier P, Giles TD, Bray GA, et al. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation 2006; 113:898–918. - PubMed
-
- Klein S, Burke LE, Bray GA, et al. Clinical implications of obesity with specific focus on cardiovascular disease: a statement for professionals from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: endorsed by the American College of Cardiology Foundation. Circulation 2004; 110:2952–2967. - PubMed
-
- Li Z, Guo X, Zheng L, et al. Grim status of hypertension in rural China: results from Northeast China Rural Cardiovascular Health Study 2013. J Am Soc Hypertens 2015; 9:358–364. - PubMed
-
- Ezzati M, Lopez AD, Rodgers A, et al. Selected major risk factors and global and regional burden of disease. Lancet 2002; 360:1347–1360. - PubMed
-
- Lu Y, Hajifathalian K, Ezzati M, et al. Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration (BMI Mediated Effects). Metabolic mediators of the effects of body-mass index, overweight, and obesity on coronary heart disease and stroke: a pooled analysis of 97 prospective cohorts with 1.8 million participants. Lancet 2014; 383:970–983. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
