

First-in-human randomized study of bimekizumab, a humanized monoclonal antibody and selective dual inhibitor of IL-17A and IL-17F, in mild psoriasis
- PMID: 27859546
- PMCID: PMC5401985
- DOI: 10.1111/bcp.13185
First-in-human randomized study of bimekizumab, a humanized monoclonal antibody and selective dual inhibitor of IL-17A and IL-17F, in mild psoriasis
Abstract
Aims: To assess safety, pharmacokinetics (PK) and clinical efficacy of bimekizumab (formerly UCB4940), a novel humanized monoclonal antibody and dual inhibitor of interleukin (IL)-17A and IL-17F, in subjects with mild plaque psoriasis.
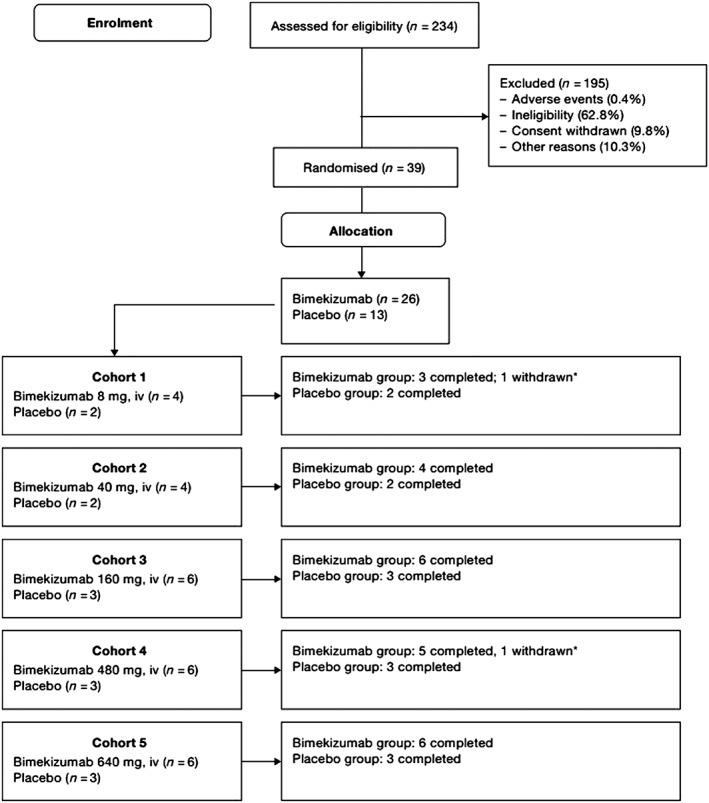
Methods: Randomized, double-blind, first-in-human study of bimekizumab in 39 subjects who received single-dose intravenous bimekizumab (8-640 mg) or placebo (NCT02529956).
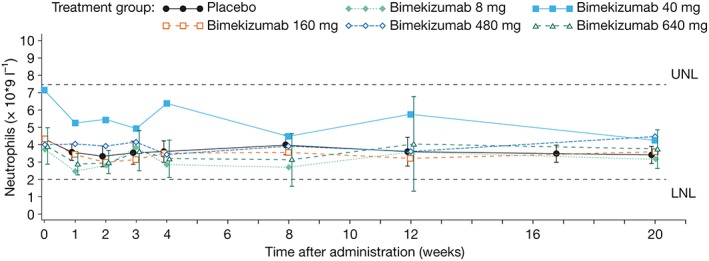
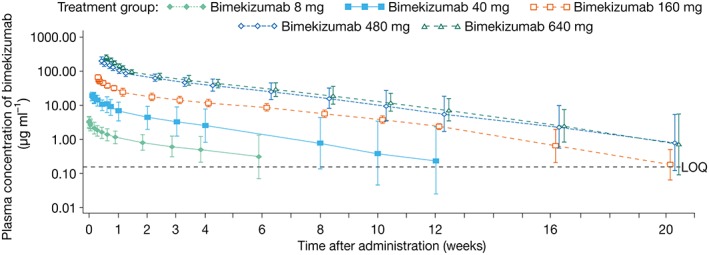
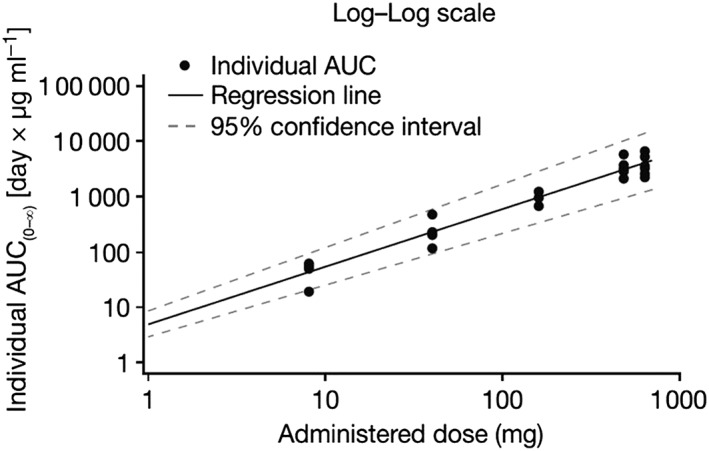
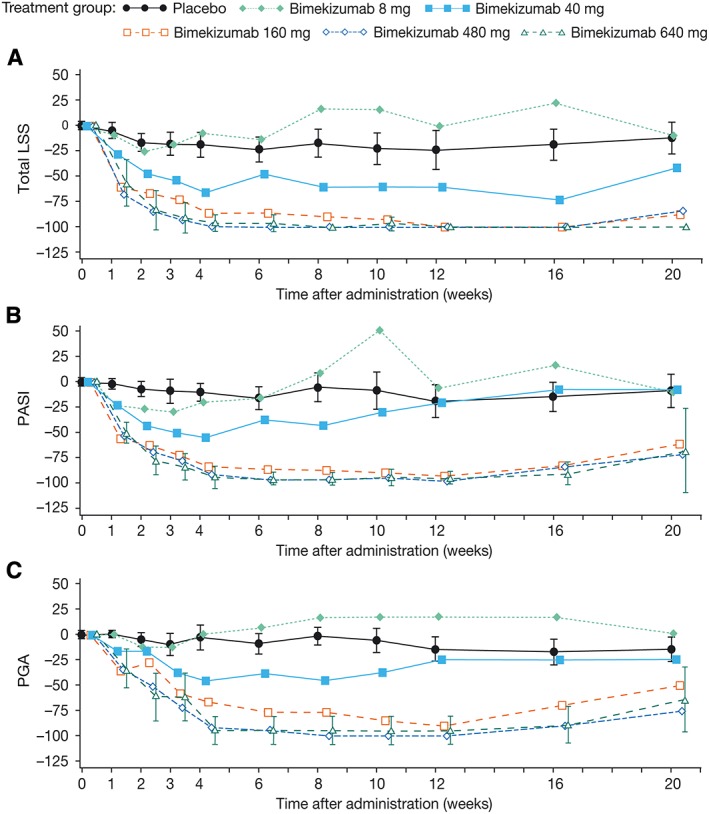
Results: Bimekizumab demonstrated dose-proportional linear PK and was tolerated across the dose range assessed. No subject discontinued due to treatment-emergent adverse events and no severe adverse events were reported. Bimekizumab demonstrated fast onset of clinically-meaningful effects on skin of patients with mild psoriasis as early as Week 2. Maximal improvements (100% or near 100% reductions from baseline) in all measures of disease activity were observed between Weeks 8-12 in subjects receiving 160-640 mg bimekizumab. The duration of effect at doses ≥160 mg was evident up to Weeks 12-20 after a single intravenous dose, dependent on endpoint.
Conclusions: This is the first study to demonstrate the safety, tolerability and clinical efficacy of a dual IL-17A and IL-17F inhibitor, in subjects with mild psoriasis. Bimekizumab showed fast onset of clinically-meaningful efficacy by Week 2, with a maximal or near-maximal magnitude of response that was maintained up to study Weeks 12-20. These findings support the continued clinical development of bimekizumab for diseases mediated by both IL-17A and IL-17F, including psoriasis.
Keywords: UCB4940; anti-IL17A; anti-IL17F; bimekizumab; interleukin-17; psoriasis.
© 2016 UCB BIOPHARMA SPRL. The British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
