

Early initiation of renal replacement treatment in patients with acute kidney injury: A systematic review and meta-analysis
- PMID: 27861388
- PMCID: PMC5120945
- DOI: 10.1097/MD.0000000000005434
Early initiation of renal replacement treatment in patients with acute kidney injury: A systematic review and meta-analysis
Abstract
Background: Acute kidney injury (AKI) is associated with a substantially increased risk of mortality for many hospitalized patients. It has been suggested that early initiation of renal replacement treatment has a favorable outcome in critically ill patients complicated with AKI. However, results of studies evaluating the effect of early initiation strategy of renal replacement treatment on AKI have been controversial and contradictory. The aim of this meta-analysis is to examine the effect of early initiation of renal replacement treatment on patients with AKI.
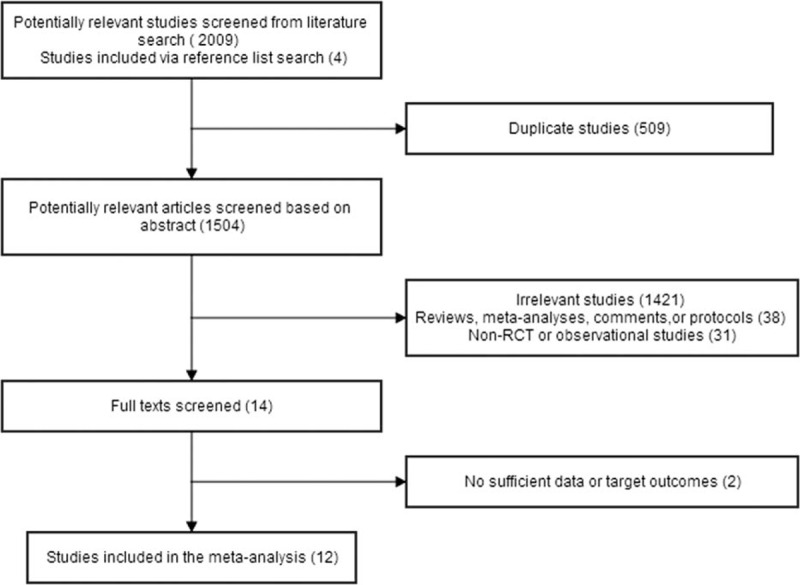
Methods: The authors searched relevant studies in PubMed, EMBASE, and the Cochrane Library through August 2016. We searched for all eligible randomized controlled trials with regard to the role of early initiation of renal replacement treatment in mortality among patients with AKI. We extracted the following information from each study: mortality, length of stay in intensive care unit (ICU), and length of stay in hospital. Random and fixed effect models were used for pooling data.
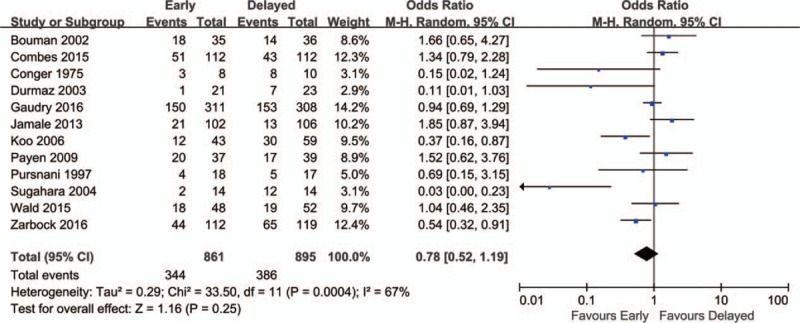
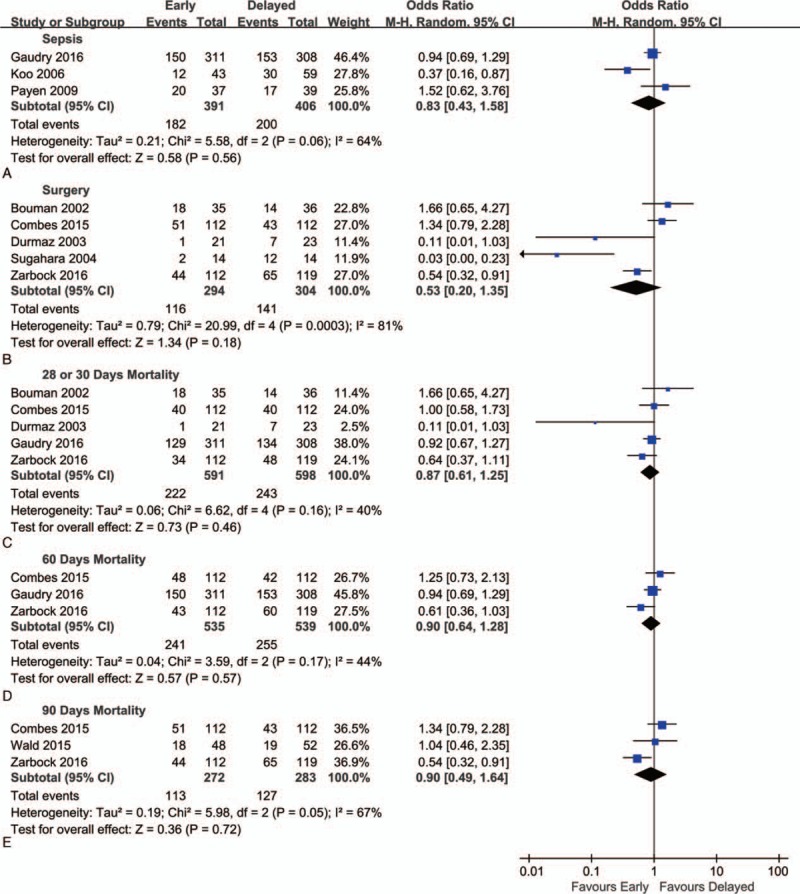
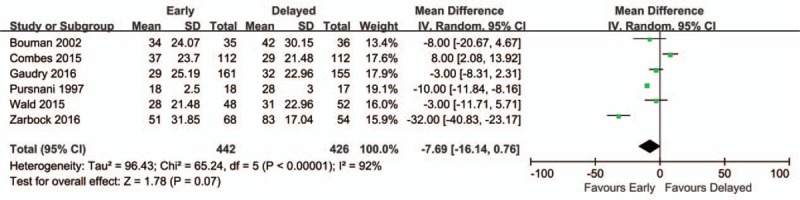
Results: Twelve trials including 1756 patients were included. The results of this meta-analysis showed that there was no significant difference between the mortality of early and delayed strategy for the initiation of renal replacement treatment using the random effect model (odds ratio = 0.78; 95% confidence interval [CI], 0.52-1.19; P = 0.25), with wild heterogeneity (chi = 33.50; I = 67%). Analyses from subgroup sepsis and postsurgery came to similar results. In addition, compared with delayed initiation strategy, early initiation showed no significant advantage in length of stay in ICU (mean difference = -0.80; 95% CI, -2.59 to 0.99; P = 0.56) and length of stay in hospital (mean difference = -7.69; 95% CI, -16.14 to 0.76; P = 0.07).
Conclusion: According to the results from present meta-analysis, early initiation of renal replacement treatment showed no survival benefits in patients with AKI. To achieve optimal timing of renal replacement treatment, further large multicenter randomized trials, with widely accepted and standardized definition of early initiation, are still needed.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Timing of renal replacement therapy initiation for acute kidney injury in critically ill patients: a systematic review of randomized clinical trials with meta-analysis and trial sequential analysis.Crit Care. 2021 Jan 6;25(1):15. doi: 10.1186/s13054-020-03451-y. Crit Care. 2021. PMID: 33407756 Free PMC article.
-
Early versus late initiation of renal replacement therapy in patients with acute kidney injury-a systematic review & meta-analysis of randomized controlled trials.BMC Nephrol. 2017 Feb 28;18(1):78. doi: 10.1186/s12882-017-0486-9. BMC Nephrol. 2017. PMID: 28245793 Free PMC article.
-
Delayed versus early initiation of renal replacement therapy for severe acute kidney injury: a systematic review and individual patient data meta-analysis of randomised clinical trials.Lancet. 2020 May 9;395(10235):1506-1515. doi: 10.1016/S0140-6736(20)30531-6. Epub 2020 Apr 23. Lancet. 2020. PMID: 32334654
-
Effect of Early vs Delayed Initiation of Renal Replacement Therapy on Mortality in Critically Ill Patients With Acute Kidney Injury: The ELAIN Randomized Clinical Trial.JAMA. 2016 May 24-31;315(20):2190-9. doi: 10.1001/jama.2016.5828. JAMA. 2016. PMID: 27209269 Clinical Trial.
-
Time to Initiation of Renal Replacement Therapy Among Critically Ill Patients With Acute Kidney Injury: A Current Systematic Review and Meta-Analysis.Crit Care Med. 2021 Aug 1;49(8):e781-e792. doi: 10.1097/CCM.0000000000005018. Crit Care Med. 2021. PMID: 33861550
Cited by
-
Early versus late initiation of renal replacement therapy for acute kidney injury in critically ill patients: A systematic review and meta-analysis.PLoS One. 2019 Oct 24;14(10):e0223493. doi: 10.1371/journal.pone.0223493. eCollection 2019. PLoS One. 2019. PMID: 31647828 Free PMC article.
-
The efficacy of renal replacement therapy strategies for septic-acute kidney injury: A PRISMA-compliant network meta-analysis.Medicine (Baltimore). 2019 Apr;98(16):e15257. doi: 10.1097/MD.0000000000015257. Medicine (Baltimore). 2019. PMID: 31008965 Free PMC article.
-
Microenvironment derived from metanephros transplantation inhibits the progression of acute kidney injury in glycerol-induced rat models.Ren Fail. 2020 Nov;42(1):89-97. doi: 10.1080/0886022X.2019.1708393. Ren Fail. 2020. PMID: 31900008 Free PMC article.
References
-
- Hoste EA, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med 2015; 41:1411–1423. - PubMed
-
- Mehta RL, Cerda J, Burdmann EA, et al. International Society of Nephrology's 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): a human rights case for nephrology. Lancet 2015; 385:2616–2643. - PubMed
-
- Gaudry S, Hajage D, Schortgen F, et al. Initiation strategies for renal-replacement therapy in the intensive care unit. N Engl J Med 2016; 375:122–133. - PubMed
-
- Lins RL, Elseviers MM, Van der Niepen P, et al. Intermittent versus continuous renal replacement therapy for acute kidney injury patients admitted to the intensive care unit: results of a randomized clinical trial. Nephrol Dial Transplant 2009; 24:512–518. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
