

Characteristics of hearing loss in patients with herpes zoster oticus
- PMID: 27861389
- PMCID: PMC5120946
- DOI: 10.1097/MD.0000000000005438
Characteristics of hearing loss in patients with herpes zoster oticus
Abstract
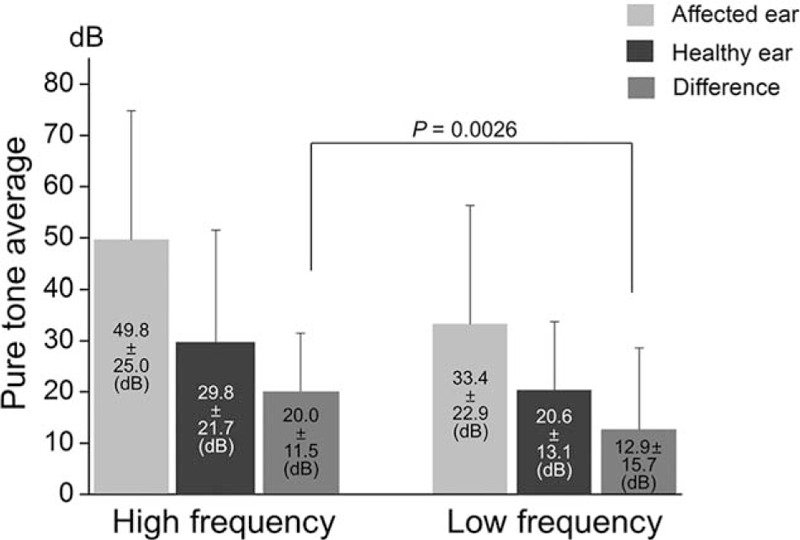
Patients with herpes zoster oticus (HZO) may commonly show symptoms associated with 7th and 8th cranial nerve (CN VII and CN VIII) dysfunction. The aim of this study is to investigate the characteristics of hearing loss in patients with HZO and discuss possible mechanisms.Ninety-five HZO patients who showed at least one of the symptoms of CN VII and CN VIII dysfunction between January 2007 and October 2014 were included in this study. Hearing loss was defined when the mean thresholds of pure tone audiometry (PTA) in speech frequency (0.5 kHz + 1 kHz + 2 kHz/3) or isolated high frequency (4 kHz + 8 kHz/2) were greater than 10 dB in the affected ear compared with the healthy ear, and a total of 72 patients were classified as the hearing loss group.The difference of mean PTA thresholds between affected and healthy ears was significantly greater in the high frequency range than in low range (20.0 ± 11.5 dB vs. 12.9 ± 15.7 dB, P = 0.0026) in patients with hearing loss (n = 72). The difference between affected and healthy ear was significantly greater in patients with vertigo (n = 34) than those without vertigo (n = 38) in both the high (P = 0.033) and low (P = 0.024) frequency ranges. In contrast, the differences between affected and healthy ears were not significantly different between patients with facial palsy (n = 50) and those without facial palsy (n = 22) in both the high (P = 0.921) and low (P = 0.382) frequency ranges.In patients with HZO, hearing loss is more severe in the high frequency range than in the low frequency range. Hearing impairment is more severe in patients with vertigo than in those without vertigo in both the high and low frequency ranges, even though the degree of hearing impairment is not significantly different between patients with and without facial palsy. These findings indicate that the mechanisms of viral spread from CN VII to CN VIII may differ between vestibular and audiologic deficits.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures




Similar articles
-
Cochleo-Vestibular Disorders in Herpes Zoster Oticus: A Literature Review and a Case of Bilateral Vestibular Hypofunction in Unilateral HZO.J Clin Med. 2023 Sep 26;12(19):6206. doi: 10.3390/jcm12196206. J Clin Med. 2023. PMID: 37834852 Free PMC article. Review.
-
Clinical manifestations in patients with herpes zoster oticus.Eur Arch Otorhinolaryngol. 2016 Jul;273(7):1739-43. doi: 10.1007/s00405-015-3756-9. Epub 2015 Aug 26. Eur Arch Otorhinolaryngol. 2016. PMID: 26308524
-
The clinical significance of findings obtained on 3D-FLAIR MR imaging in patients with Ramsay-Hunt syndrome.Laryngoscope. 2015 Apr;125(4):950-5. doi: 10.1002/lary.24973. Epub 2014 Oct 27. Laryngoscope. 2015. PMID: 25346250
-
Statistical analysis of pure tone audiometry and caloric test in herpes zoster oticus.Clin Exp Otorhinolaryngol. 2008 Mar;1(1):15-9. doi: 10.3342/ceo.2008.1.1.15. Epub 2008 Mar 20. Clin Exp Otorhinolaryngol. 2008. PMID: 19434256 Free PMC article.
-
Vestibulocochlear nerve.Semin Neurol. 2009 Feb;29(1):66-73. doi: 10.1055/s-0028-1124024. Epub 2009 Feb 12. Semin Neurol. 2009. PMID: 19214934 Review.
Cited by
-
[Clinical and therapeutic features of herpes zoster oticus: a case report].Pan Afr Med J. 2022 Mar 3;41:171. doi: 10.11604/pamj.2022.41.171.33711. eCollection 2022. Pan Afr Med J. 2022. PMID: 35573434 Free PMC article. Review. French.
-
Atypical clinical manifestations of herpes zoster oticus: diagnostic usefulness of magnetic resonance imaging.J Neurovirol. 2019 Dec;25(6):874-882. doi: 10.1007/s13365-019-00781-8. Epub 2019 Jul 5. J Neurovirol. 2019. PMID: 31278535
-
Effect of Herpes Zoster Treatment and Sudden Sensorineural Hearing Loss Using National Health Insurance Claims Data of South Korea.Medicina (Kaunas). 2023 Apr 20;59(4):808. doi: 10.3390/medicina59040808. Medicina (Kaunas). 2023. PMID: 37109766 Free PMC article.
-
Cochleo-Vestibular Disorders in Herpes Zoster Oticus: A Literature Review and a Case of Bilateral Vestibular Hypofunction in Unilateral HZO.J Clin Med. 2023 Sep 26;12(19):6206. doi: 10.3390/jcm12196206. J Clin Med. 2023. PMID: 37834852 Free PMC article. Review.
-
Varicella-zoster virus vasculopathy: a rare complication of Ramsay Hunt Syndrome: a literature review.Front Neurol. 2025 Jun 19;16:1509110. doi: 10.3389/fneur.2025.1509110. eCollection 2025. Front Neurol. 2025. PMID: 40612802 Free PMC article.
References
-
- Blackley B, Friedmann I, Wright I. Herpes zoster auris associated with facial nerve palsy and auditory nerve symptoms: a case report with histopathological findings. Acta Otolaryngol 1967; 63:533–550. - PubMed
-
- Elliott KJ. Other neurological complications of herpes zoster and their management. Ann Neurol 1994; 35 (Suppl):S57–S61. - PubMed
-
- Kaberos A, Balatsouras DG, Korres SG, et al. Audiological assessment in Ramsay Hunt syndrome. Ann Otol Rhinol Laryngol 2002; 111:68–76. - PubMed
-
- Kuhweide R, Van de Steene V, Vlaminck S, et al. Ramsay Hunt syndrome: pathophysiology of cochleovestibular symptoms. J Laryngol Otol 2002; 116:844–848. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
