

Effect of Cognitively Stimulating Activities on Symptom Management of Delirium Superimposed on Dementia: A Randomized Controlled Trial
- PMID: 27861718
- PMCID: PMC5173415
- DOI: 10.1111/jgs.14511
Effect of Cognitively Stimulating Activities on Symptom Management of Delirium Superimposed on Dementia: A Randomized Controlled Trial
Abstract
Objective: To determine whether cognitively stimulating activities would reduce duration and severity of delirium and improve cognitive and physical function to a greater extent than usual care.
Design: Single-blind randomized clinical trial.
Setting: Eight post-acute care (PAC) facilities.
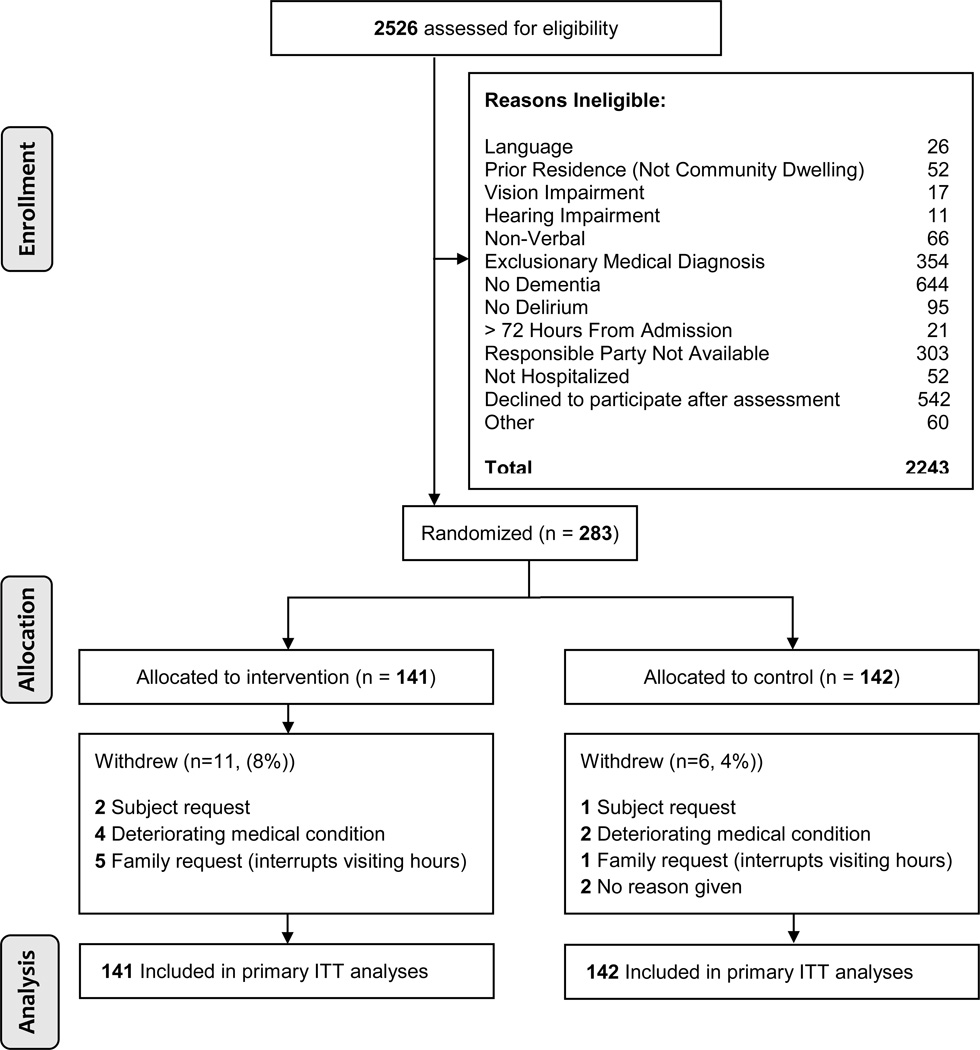
Participants: Community-dwelling older adults with dementia and delirium (N = 283).
Intervention: Research staff provided cognitively stimulating activities daily for up to 30 days.
Measurements: Primary outcomes were delirium duration (Confusion Assessment Method) and delirium severity (Delirium Rating Scale). Secondary outcomes were cognitive function (Digits Forward, Montreal Cognitive Assessment, CLOX) and physical function (Barthel Index).
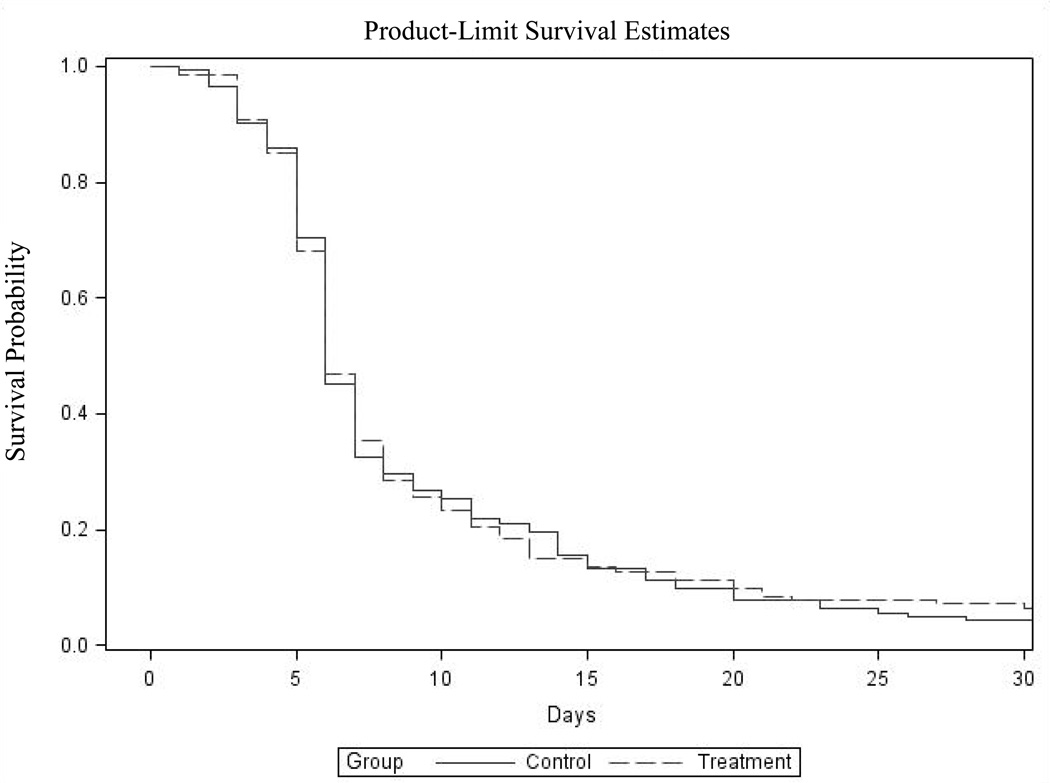
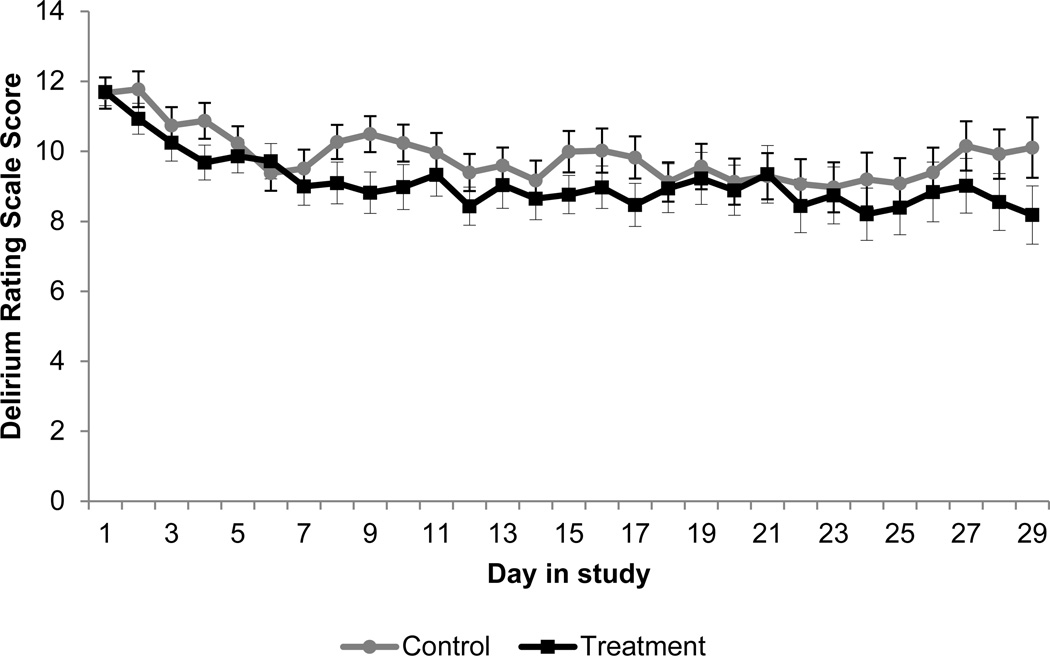
Results: Mean percentage of delirium-free days (intervention: 64.8%, 95% confidence interval (CI) = 59.6-70.1; control: 68.7%, 95% CI = 63.9-73.6; P = .37, Wilcoxon rank sum test) and delirium severity (range 0-39: intervention: 10.77, 95% CI = 10.10-11.45; control: 11.15, 95% CI = 10.50-11.80; difference 0.37, 95% CI = 0.56-1.31, P = .43) were similar in both groups. Significant differences for secondary outcomes favoring intervention were found (executive function (range 0-15): intervention: 6.58, 95% CI = 6.12-7.04; control: 5.89, 95% CI = 5.45-6.33; difference -0.69, 95% CI = 1.33 to -0.06, P = .03; constructional praxis (range 0-15): intervention: 8.84, 95% CI = 8.83-9.34; control: 7.53, 95% CI = 7.04-8.01; difference -1.31, 95% CI = 2.01 to -0.61, P < .001). After adjusting for baseline constructional praxis, the group comparison was no longer significant. Average length of stay was shorter in the intervention (36.09 days) than the control (53.13 days) group (standard error = 0.15, P = .01, negative binomial regression).
Conclusion: Cognitively stimulating activities did not improve delirium but improved executive function and reduced length of stay. Resolution of delirium may require more-intense nonpharmacological management when the individual has dementia.
Keywords: delirium; dementia; nonpharmacological intervention; postacute care.
© 2016, Copyright the Authors Journal compilation © 2016, The American Geriatrics Society.
Figures
References
-
- Fick DM, Agostini JV, Inouye SK. Delirium superimposed on dementia: A systematic review. J Am Geriatr Soc. 2002;50(10):1723–1732. - PubMed
-
- Mark RE, Muselaers N, Scholten H, et al. Short-term cognitive effects after recovery from a delirium in a hospitalized elderly sample. J Nerv Ment Dis. 2014;202(10):732–737. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
