

Beta-Blocker Use in U.S. Nursing Home Residents After Myocardial Infarction: A National Study
- PMID: 27861719
- PMCID: PMC5397324
- DOI: 10.1111/jgs.14671
Beta-Blocker Use in U.S. Nursing Home Residents After Myocardial Infarction: A National Study
Abstract
Objectives: To evaluate how often beta-blockers were started after acute myocardial infarction (AMI) in nursing home (NH) residents who previously did not use these drugs and to evaluate which factors were associated with post-AMI use of beta-blockers.
Design: Retrospective cohort using linked national Minimum Data Set assessments; Online Survey, Certification and Reporting records; and Medicare claims.
Setting: U.S. NHs.
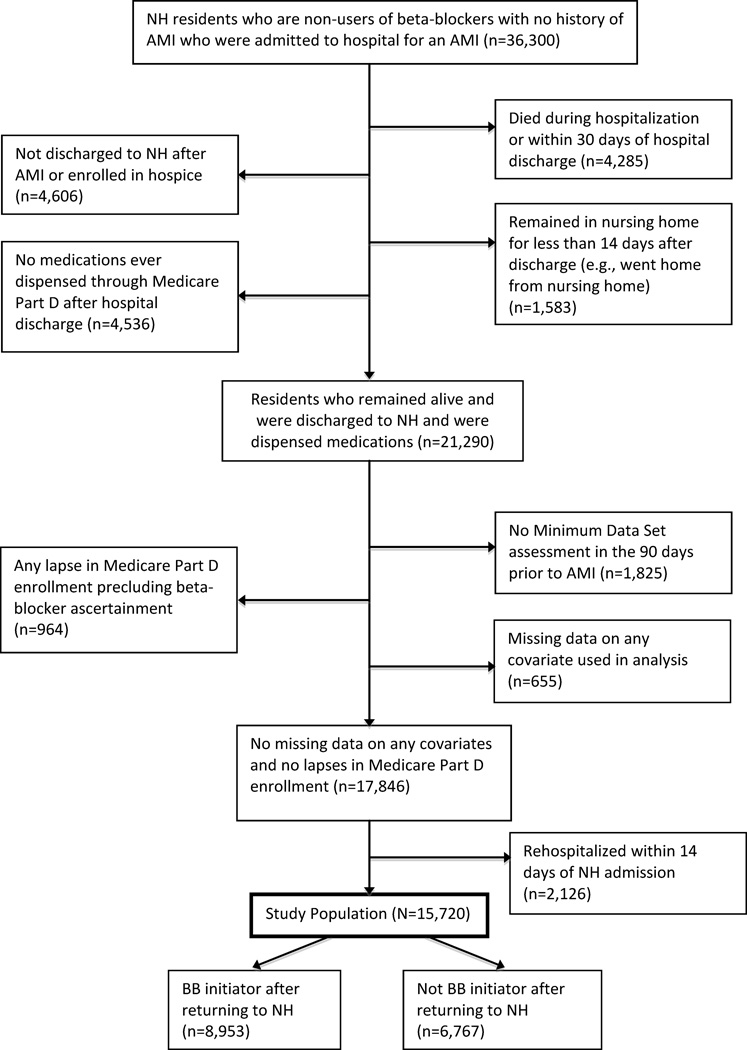
Participants: National cohort of 15,720 residents aged 65 and older who were hospitalized for AMI between May 2007 and March 2010, had not taken beta-blockers for at least 4 months before their AMI, and survived 14 days or longer after NH readmission.
Measurements: The outcome was beta-blocker initiation within 30 days of NH readmission.
Results: Fifty-seven percent (n = 8,953) of residents initiated a beta-blocker after AMI. After covariate adjustment, use of beta-blockers was less in older residents (ranging from odds ratio (OR) = 0.89, 95% confidence interval (CI) = 0.79-1.00 for aged 75-84 to OR = 0.65, 95% CI = 0.54-0.79 for ≥95 vs 65-74) and less in residents with higher levels of functional impairment (dependent or totally dependent vs independent to limited assistance: OR = 0.84, 95% CI = 0.75-0.94) and medication use (≥15 vs ≤10 medications: OR = 0.89, 95% CI = 0.80-0.99). A wide variety of resident and NH characteristics were not associated with beta-blocker use, including sex, cognitive function, comorbidity burden, and NH ownership.
Conclusion: Almost half of older NH residents in the United States do not initiate a beta-blocker after AMI. The absence of observed factors that strongly predict beta-blocker use may indicate a lack of consensus on how to manage older NH residents, suggesting the need to develop and disseminate thoughtful practice standards.
Keywords: beta-blockers; drug utilization; elderly; myocardial infarction; nursing homes.
© 2016, Copyright the Authors Journal compilation © 2016, The American Geriatrics Society.
Figures
Similar articles
-
Beta-Blockers for the Secondary Prevention of Myocardial Infarction in People with Dementia: A Systematic Review.J Alzheimers Dis. 2019;71(4):1105-1114. doi: 10.3233/JAD-190503. J Alzheimers Dis. 2019. PMID: 31476156 Free PMC article.
-
Secondary Prevention Medication Use After Myocardial Infarction in U.S. Nursing Home Residents.J Am Geriatr Soc. 2017 Nov;65(11):2397-2404. doi: 10.1111/jgs.15144. Epub 2017 Oct 17. J Am Geriatr Soc. 2017. PMID: 29044457 Free PMC article.
-
National use and effectiveness of beta-blockers for the treatment of elderly patients after acute myocardial infarction: National Cooperative Cardiovascular Project.JAMA. 1998 Aug 19;280(7):623-9. doi: 10.1001/jama.280.7.623. JAMA. 1998. PMID: 9718054
-
Association of β-Blockers With Functional Outcomes, Death, and Rehospitalization in Older Nursing Home Residents After Acute Myocardial Infarction.JAMA Intern Med. 2017 Feb 1;177(2):254-262. doi: 10.1001/jamainternmed.2016.7701. JAMA Intern Med. 2017. PMID: 27942713 Free PMC article.
-
Under-utilisation of beta-blockers after acute myocardial infarction. Pharmacoeconomic implications.Pharmacoeconomics. 1999 Mar;15(3):257-68. doi: 10.2165/00019053-199915030-00005. Pharmacoeconomics. 1999. PMID: 10537433 Review.
Cited by
-
Association Between Secondary Prevention Medication Use and Outcomes in Frail Older Adults After Acute Myocardial Infarction.Circ Cardiovasc Qual Outcomes. 2019 Apr;12(4):e004942. doi: 10.1161/CIRCOUTCOMES.118.004942. Circ Cardiovasc Qual Outcomes. 2019. PMID: 31002274 Free PMC article.
-
Comparative Effectiveness of Angiotensin II Receptor Blockers and Angiotensin-Converting Enzyme Inhibitors in Older Nursing Home Residents After Myocardial Infarction: A Retrospective Cohort Study.Drugs Aging. 2020 Oct;37(10):755-766. doi: 10.1007/s40266-020-00791-w. Drugs Aging. 2020. PMID: 32808250 Free PMC article.
-
Beta-Blockers for the Secondary Prevention of Myocardial Infarction in People with Dementia: A Systematic Review.J Alzheimers Dis. 2019;71(4):1105-1114. doi: 10.3233/JAD-190503. J Alzheimers Dis. 2019. PMID: 31476156 Free PMC article.
-
Comparing Outcomes Between Thiazide Diuretics and Other First-line Antihypertensive Drugs in Long-term Nursing Home Residents.Clin Ther. 2020 Apr;42(4):583-591. doi: 10.1016/j.clinthera.2020.02.016. Epub 2020 Mar 27. Clin Ther. 2020. PMID: 32229030 Free PMC article.
-
Patient-Important Adverse Events of β-blockers in Frail Older Adults after Acute Myocardial Infarction.J Gerontol A Biol Sci Med Sci. 2019 Jul 12;74(8):1277-1281. doi: 10.1093/gerona/gly191. J Gerontol A Biol Sci Med Sci. 2019. PMID: 30137259 Free PMC article.
References
-
- Khera S, Kolte D, Gupta T, Mujib M, Aronow WS, Agarwal P, et al. Management and outcomes of ST-elevation myocardial infarction in nursing home versus community-dwelling older patients: a propensity matched study. Journal of the American Medical Directors Association. 2014;15(8):593–599. - PubMed
-
- Rich MW, Chyun DA, Skolnick AH, Alexander KP, Forman DE, Kitzman DW, et al. Knowledge Gaps in Cardiovascular Care of the Older Adult Population: A Scientific Statement From the American Heart Association, American College of Cardiology, and American Geriatrics Society. Journal of the American College of Cardiology. 2016;67(20):2419–2440. - PMC - PubMed
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE, Jr, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):529–555. - PubMed
-
- Smith SC, Jr, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, et al. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and other Atherosclerotic Vascular Disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation. 2011;124(22):2458–2473. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
