

Pathology-based staging for HPV-positive squamous carcinoma of the oropharynx
- PMID: 27865363
- PMCID: PMC5523818
- DOI: 10.1016/j.oraloncology.2016.09.004
Pathology-based staging for HPV-positive squamous carcinoma of the oropharynx
Abstract
Objective: The rapid worldwide rise in incidence of human papillomavirus (HPV)-positive oropharyngeal squamous cell carcinoma (OPSCC) has generated studies confirming this disease as an entity distinct from traditional OPSCC. Based on pathology, surgical studies have revealed prognosticators specific to HPV-positive OPSCC. The current AJCC/UICC staging and pathologic nodal (pN)-classification do not differentiate for survival, demonstrating the need for new, HPV-specific OPSCC staging. The objective of this study was to define a pathologic staging system specific to HPV-positive OPSCC.
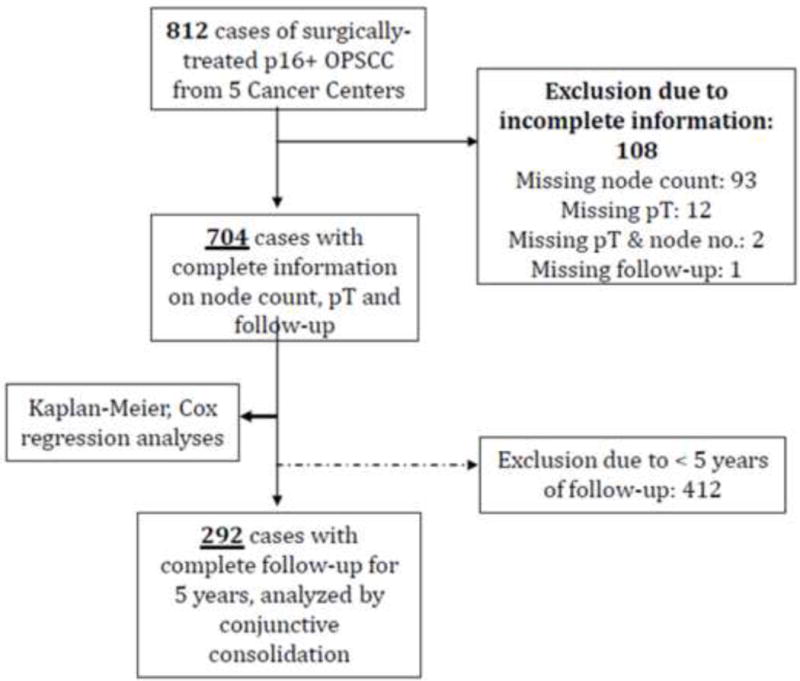
Methods: Data were assembled from a surgically-managed, p16-positive OPSCC cohort (any T, any N, M0) of 704 patients from five cancer centers. Analysis was performed for (a) the AJCC/UICC pathologic staging, (b) newly published clinical staging for non-surgically managed HPV-positive OPSCC, and (c) a novel, pathology-based, "HPVpath" staging system that combines features of the primary tumor and nodal metastases.
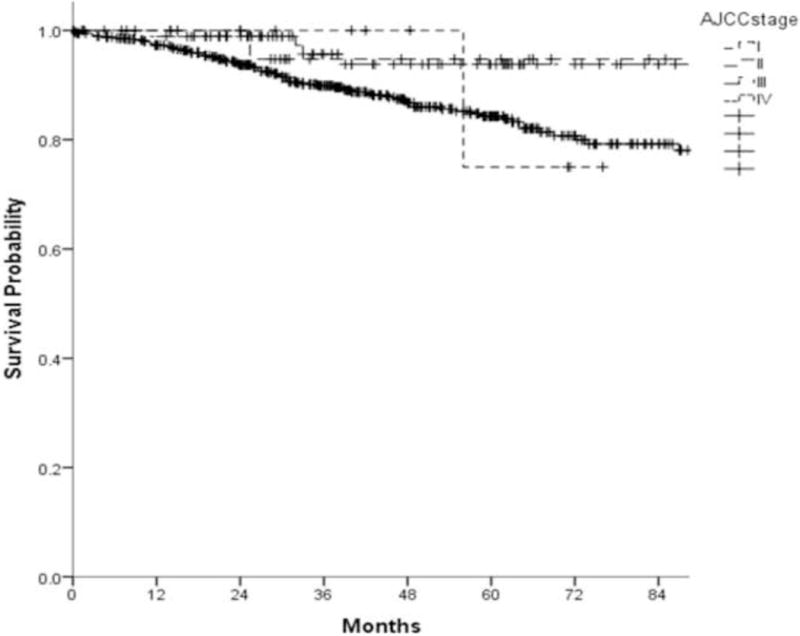
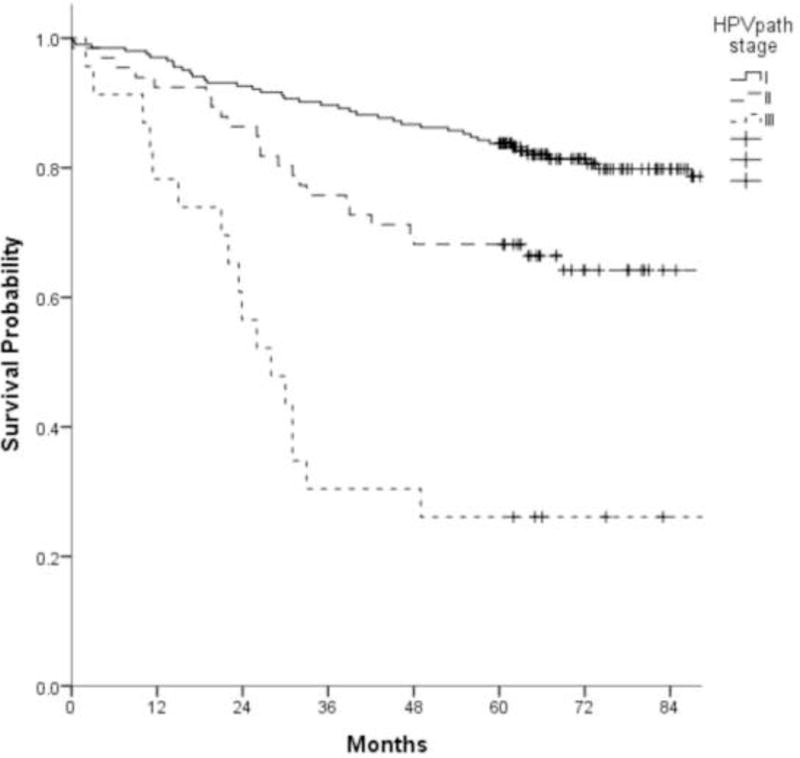
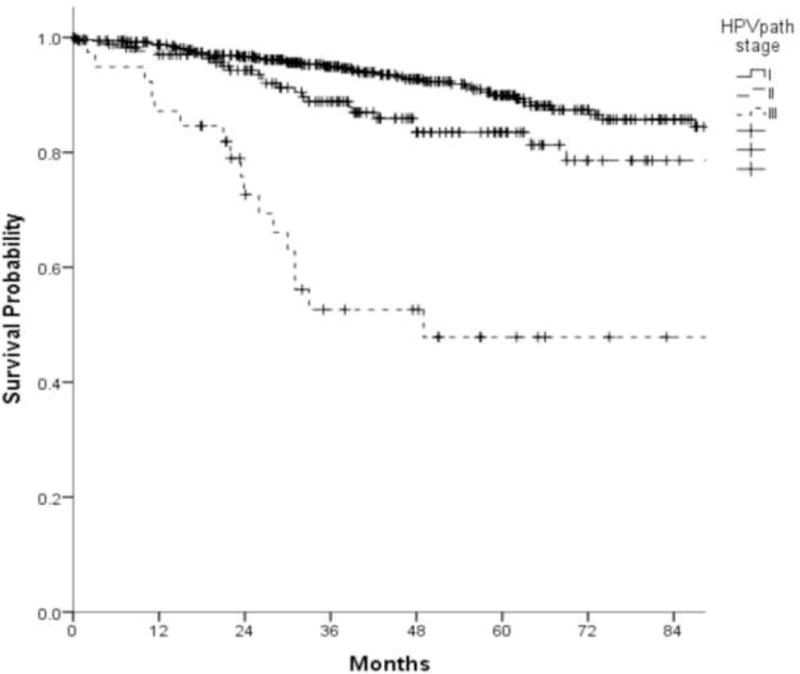
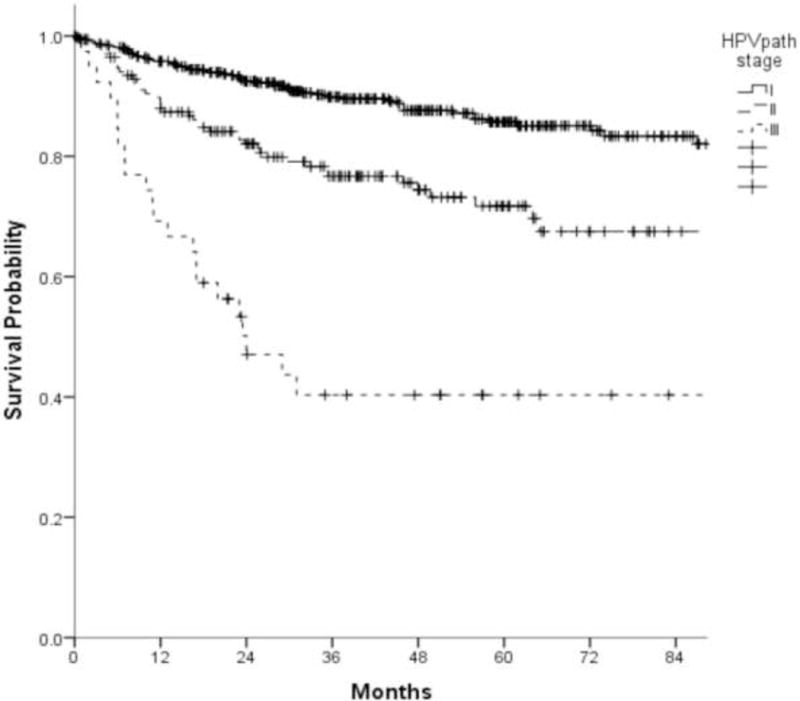
Results: A combination of AJCC/UICC pT-classification and pathology-confirmed metastatic node count (⩽4 versus ⩾5) yielded three groups: stages I (pT1-T2, ⩽4 nodes), II (pT1-T2, ⩾5 nodes; pT3-T4, ⩽4 nodes), and III (pT3-T4, ⩾5 nodes), with incrementally worse prognosis (Kaplan-Meier overall survival of 90%, 84% and 48% respectively). Existing AJCC/UICC pathologic staging lacked prognostic definition. Newly published HPV-specific clinical stagings from non-surgically managed patients, although prognostic, showed lower precision for this surgically managed cohort.
Conclusions: Three loco-regional "HPVpath" stages are identifiable for HPV-positive OPSCC, based on a combination of AJCC/UICC primary tumor pT-classification and metastatic node count. A workable, pathologic staging system is feasible to establish prognosis and guide adjuvant therapy decisions in surgically-managed HPV-positive OPSCC.
Keywords: Head and neck cancer; Human papillomavirus; Oropharynx cancer; P16 gene; P16-positive; Pathologic staging; Staging.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
None of the co-authors had any conflicts of interest which could have affected the current study.
Figures
References
-
- Gillison ML. Human papillomavirus-associated head and neck cancer is a distinct epidemiologic, clinical, and molecular entity. Semin Oncol. 2004;31:744–54. - PubMed
-
- Grant DG, Salassa JR, Hinni ML, Pearson BW, Perry WC. Carcinoma of the tongue base treated by transoral laser microsurgery, part one: Untreated tumors, a prospective analysis of oncologic and functional outcomes. Laryngoscope. 2006;116:2150–5. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
