

Dysbiosis in the intensive care unit: Microbiome science coming to the bedside
- PMID: 27866110
- PMCID: PMC5328797
- DOI: 10.1016/j.jcrc.2016.09.029
Dysbiosis in the intensive care unit: Microbiome science coming to the bedside
Abstract
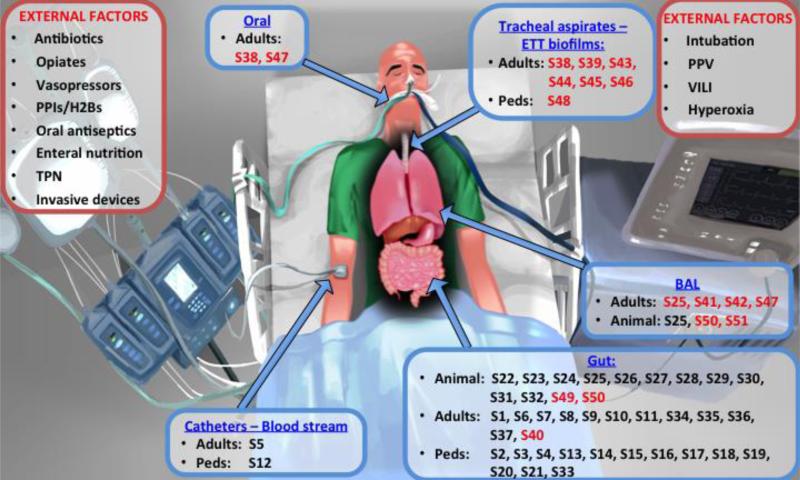
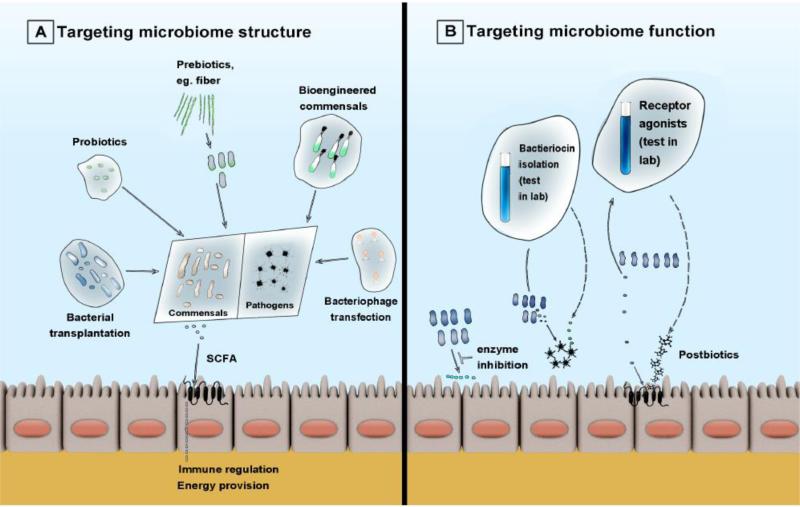
Complex microbial communities within the human body, constituting the microbiome, have a broad impact on human health and disease. A growing body of research now examines the role of the microbiome in patients with critical illness, such as sepsis and acute respiratory failure. In this article, we provide an introduction to microbiome concepts and terminology and we systematically review the current evidence base of the critical-illness microbiome, including 51 studies in animal models and pediatric and adult critically ill patients. We further examine how this emerging scientific discipline may transform the way we manage infectious and inflammatory diseases in intensive care units. The evolving molecular, culture-independent techniques offer the ability to study microbial communities in unprecedented depth and detail, and in the short-term, may enable us to diagnose and treat infections in critical care more precisely and effectively. Longer term, these tools may also give us insights in the underlying pathophysiology of critical illness and reveal previously unsuspected targets for innovative, microbiome-targeted therapeutics. We finally propose a roadmap for future studies in the field for transforming critical care from its current isolated focus on the host to a more personalized paradigm addressing both human and microbial contributions to critical illness.
Keywords: Acute respiratory distress syndrome; Acute respiratory failure; Dysbiosis; Microbiome; Microbiota; Sepsis.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Sender R, Fuchs S, Milo R. Are We Really Vastly Outnumbered? Revisiting the Ratio of Bacterial to Host Cells in Humans. Cell. 2016;164:337–40. doi:10.1016/j.cell.2016.01.013. - PubMed
-
- Gotts JE, Matthay MA. Sepsis: pathophysiology and clinical management. BMJ. 2016;353:i1585. doi:10.1136/bmj.i1585. - PubMed
-
- Barrett ML, Smith MW, Elixhauser A, Honigman LS, Pines JM. HCUP Statistical Brief #185. Agency for Healthcare Research and Quality; Rockville, MD: 2014. Utilization of Intensive Care Services, 2011. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
