

Regional Differences in the Prevalence of Cardiovascular Disease
- PMID: 27866565
- PMCID: PMC5143789
- DOI: 10.3238/arztebl.2016.0704
Regional Differences in the Prevalence of Cardiovascular Disease
Erratum in
-
Erratum.Dtsch Arztebl Int. 2017 Feb;114(7):109. doi: 10.3238/arztebl.2017.0109. Epub 2017 Feb 17. Dtsch Arztebl Int. 2017. PMID: 31305771 Free PMC article.
Abstract
Background: Cardiovascular disease continues to be the single most common cause of death and to account for the largest single portion of treatment costs in Germany. Reliable data on regional differences in the frequency of cardio - vascular disease are important for the planning of targeted care structures and preventive measures.
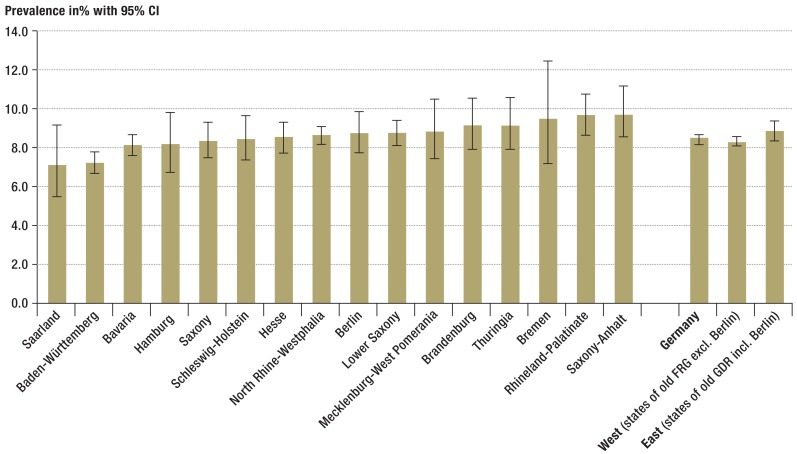
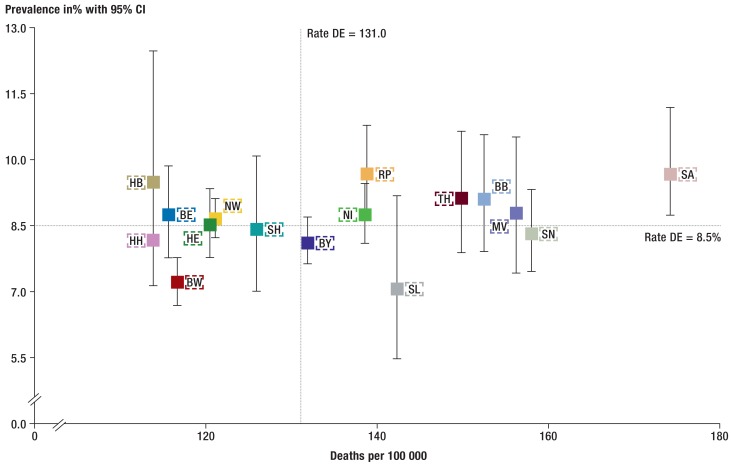
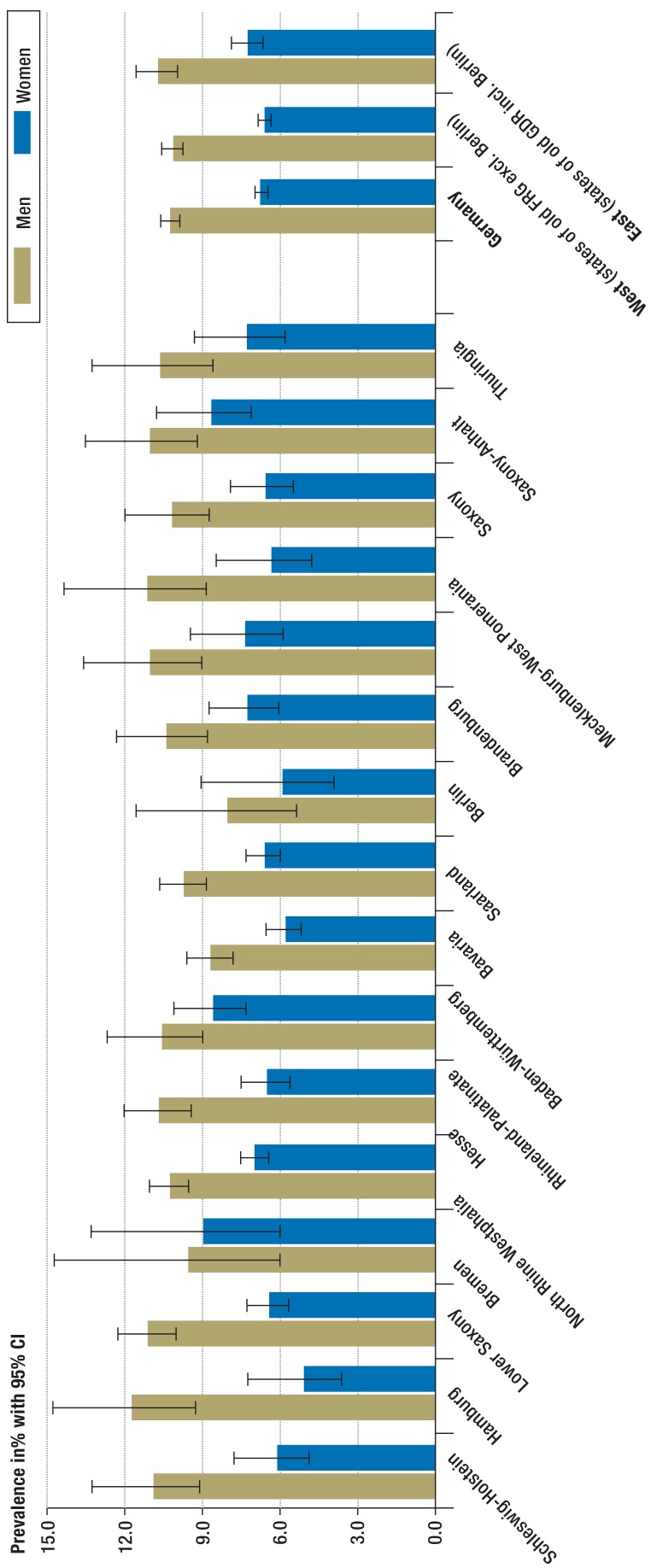
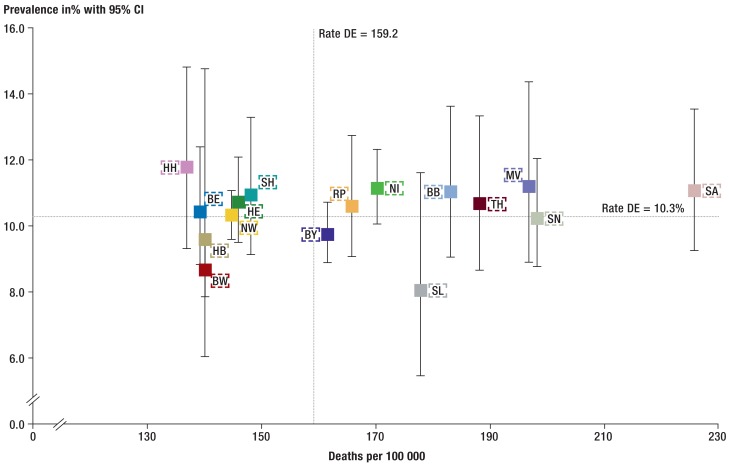
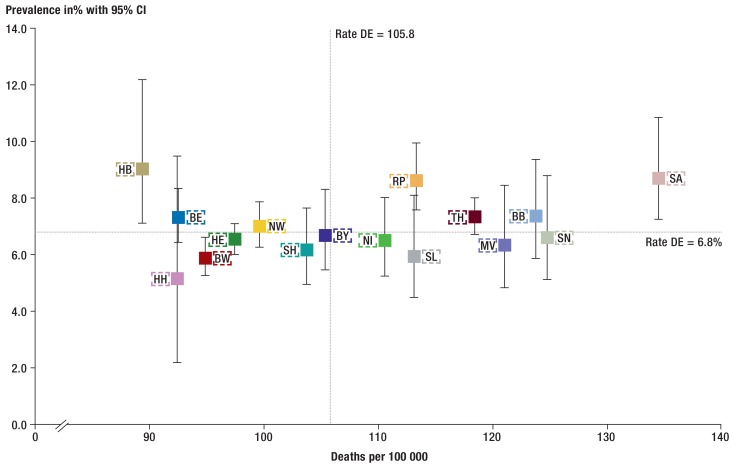
Methods: Pooled data from the German Health Update (GEDA), a nationwide telephone health survey conducted in 2009, 2010 and 2012 (n = 62 214) were used to estimate the lifetime prevalence of major cardiovascular disease (self-reported medical diagnosis of myocardial infarction, other coronary heart disease, stroke, or congestive heart failure) in each of the German federal states. The influence of sociodemographic factors on regional prevalence differences was examined in adjusted logistic regression analyses. Prevalences were compared with mortality rates from cardiovascular disease that were obtained from cause-of-death statistics.
Results: The lifetime prevalence of cardiovascular disease in Germany ranged from 10.0% in Baden-W¨rttemberg to 15.8% in Saxony-Anhalt. After adjustment for age, sex, socioeconomic status, and size of the communities of residence, nine of the other 15 states had significantly higher prevalences than Baden-W¨rttemberg, with odds ratios ranging from 1.26 (Hesse) to 1.55 (Saxony-Anhalt). Four of the five states that previously constituted the German Democratic Republic (East Germany) had above-average figures for prevalence and mortality.
Conclusion: There are relevant differences among the German federal states in the lifetime prevalence of major cardiovascular disease, which are only partly accounted for by differences in age and sex distribution, socioeconomic status, and community size.
Figures
Comment in
-
Home, Lifestyle and the Burden of Disease.Dtsch Arztebl Int. 2016 Oct 21;113(42):703. doi: 10.3238/arztebl.2016.0703. Dtsch Arztebl Int. 2016. PMID: 27866564 Free PMC article. No abstract available.
-
Questionable Validity of Data Sources.Dtsch Arztebl Int. 2017 Mar 24;114(12):211. doi: 10.3238/arztebl.2017.0211a. Dtsch Arztebl Int. 2017. PMID: 28407843 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2017 Mar 24;114(12):211. doi: 10.3238/arztebl.2017.0211b. Dtsch Arztebl Int. 2017. PMID: 28407844 Free PMC article. No abstract available.
References
-
- Robert Koch-Institut (ed.) Gesundheit in Deutschland 2015. Gesundheitsberichterstattung des Bundes. www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung... (last accessed on 7 June 2016)
-
- Gesundheitsberichterstattung des Bundes Sterbefälle, Sterbeziffern (je 100.000 Einwohner, altersstandardisiert) (ab 1998). Gliederungsmerkmale. Jahre, Region, Alter, Geschlecht, Nationalität, ICD-10, Art der Standardisierung. www.gbe-bund.de/gbe10/ (last accessed on 6 November 2015)
-
- Robert Koch-Institut. Krankheitskosten. Heft 48. Gesundheitsberichterstattung des Bundes Berlin 2009. www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung... (last accessed on 7 June 2016)
-
- Gesundheitsberichterstattung des Bundes. Diagnosedaten der Krankenhäuser ab 2000 (Fälle/Sterbefälle, Fälle je 100000 Einwohner (altersstandardisiert)) www.gbe-bund.de/gbe10/ (last accessed on 15 February 2016)
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources