

Dialysate Potassium, Serum Potassium, Mortality, and Arrhythmia Events in Hemodialysis: Results From the Dialysis Outcomes and Practice Patterns Study (DOPPS)
- PMID: 27866964
- PMCID: PMC5520979
- DOI: 10.1053/j.ajkd.2016.09.015
Dialysate Potassium, Serum Potassium, Mortality, and Arrhythmia Events in Hemodialysis: Results From the Dialysis Outcomes and Practice Patterns Study (DOPPS)
Abstract
Background: Sudden death is a leading cause of death in patients on maintenance hemodialysis therapy. During hemodialysis sessions, the gradient between serum and dialysate levels results in rapid electrolyte shifts, which may contribute to arrhythmias and sudden death. Controversies exist about the optimal electrolyte concentration in the dialysate; specifically, it is unclear whether patient outcomes differ among those treated with a dialysate potassium concentration of 3 mEq/L compared to 2 mEq/L.
Study design: Prospective cohort study.
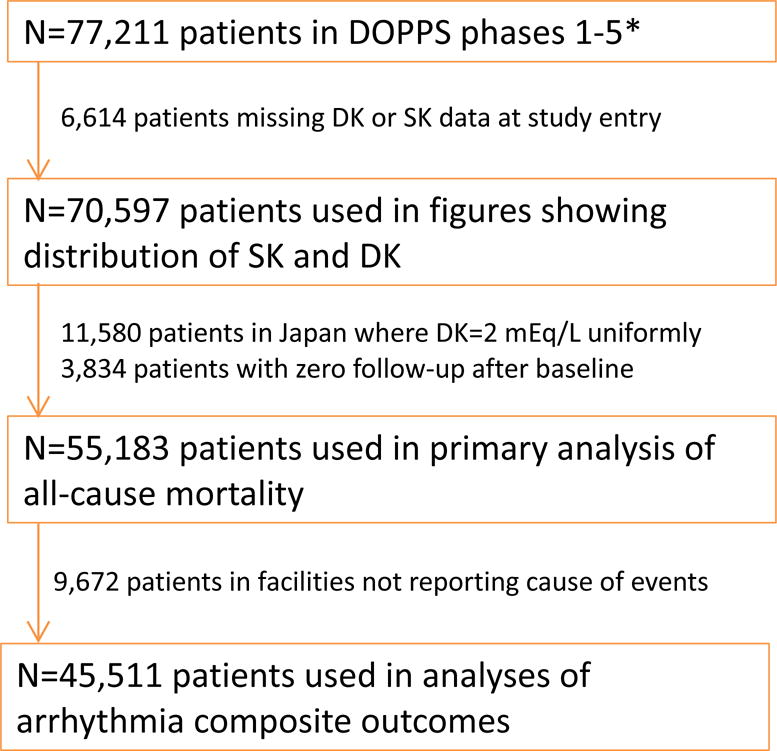
Setting & participants: 55,183 patients from 20 countries in the Dialysis Outcomes and Practice Patterns Study (DOPPS) phases 1 to 5 (1996-2015).
Predictor: Dialysate potassium concentration at study entry.
Outcomes: Cox regression was used to estimate the association between dialysate potassium concentration and both all-cause mortality and an arrhythmia composite outcome (arrhythmia-related hospitalization or sudden death), adjusting for potential confounders.
Results: During a median follow-up of 16.5 months, 24% of patients died and 7% had an arrhythmia composite outcome. No meaningful difference in clinical outcomes was observed for patients treated with a dialysate potassium concentration of 3 versus 2 mEq/L (adjusted HRs were 0.96 [95% CI, 0.91-1.01] for mortality and 0.98 [95% CI, 0.88-1.08] for arrhythmia composite). Results were similar across predialysis serum potassium levels. As in prior studies, higher serum potassium level was associated with adverse outcomes. However, dialysate potassium concentration had only minimal impact on serum potassium level measured predialysis (+0.09 [95% CI, 0.05-0.14] mEq/L serum potassium per 1 mEq/L greater dialysate potassium concentration).
Limitations: Data were not available for delivered (vs prescribed) dialysate potassium concentration and postdialysis serum potassium level; possible unmeasured confounding.
Conclusions: In combination, these results suggest that approaches other than altering dialysate potassium concentration (eg, education on dietary potassium sources and prescription of potassium-binding medications) may merit further attention to reduce risks associated with high serum potassium levels.
Keywords: Dialysate potassium; Dialysis Outcomes and Practice Patterns Study (DOPPS); arrhythmia; cardiac instability; electrolyte shift; end-stage renal disease (ESRD); hemodialysis; hyperkalemia; mortality; potassium gradient; serum potassium; sudden death.
Copyright © 2016 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Herzog CA, Mangrum JM, Passman R. Sudden cardiac death and dialysis patients. Semin Dial. 2008;21(4):300–307. - PubMed
-
- Foley RN, Gilbertson DT, Murray T, Collins AJ. Long interdialytic interval and mortality among patients receiving hemodialysis. N Engl J Med. 2011;365(12):1099–1107. - PubMed
-
- Bleyer AJ, Hartman J, Brannon PC, Reeves-Daniel A, Satko SG, Russell G. Characteristics of sudden death in hemodialysis patients. Kidney Int. 2006;69(12):2268–2273. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
