

Effect of adding intrathecal morphine to a multimodal analgesic regimen for postoperative pain management after laparoscopic bariatric surgery: a prospective, double-blind, randomized controlled trial
- PMID: 27867510
- PMCID: PMC5102100
- DOI: 10.1177/2049463716668904
Effect of adding intrathecal morphine to a multimodal analgesic regimen for postoperative pain management after laparoscopic bariatric surgery: a prospective, double-blind, randomized controlled trial
Abstract
Background: Pain control after bariatric surgery is a major challenge. Our objective was to study the efficacy and safety of intrathecal (IT) morphine 0.3 mg added to bupivacaine 0.5% for postoperative pain after laparoscopic bariatric surgery.
Methods: After local ethics committee approval, 100 morbidly obese patients scheduled for laparoscopic bariatric surgery were enrolled in this study. Patients were randomly assigned into two groups: Group I received IT 0.3 mg morphine (0.3 mL) added to 1.2 mL of bupivacaine 0.5%; Group II received IT 0.3 mL saline added to 1.2 mL of bupivacaine 0.5%, immediately before induction of general anaesthesia. For both groups, 60 mg ketorolac and 1000 mg paracetamol were infused 30 minutes before the end of surgery. After wound closure, 20 mL bupivacaine 0.25% was infiltrated at wound edges.
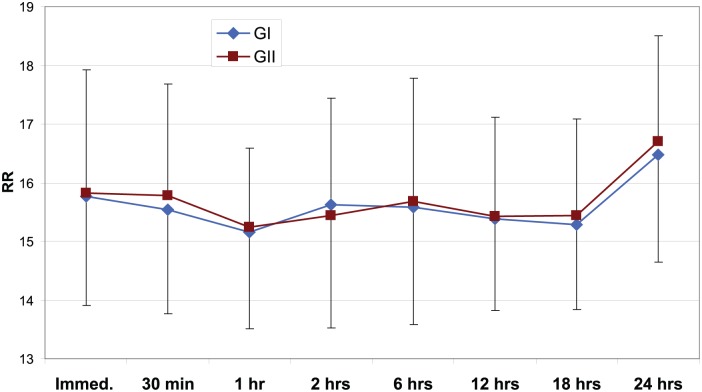
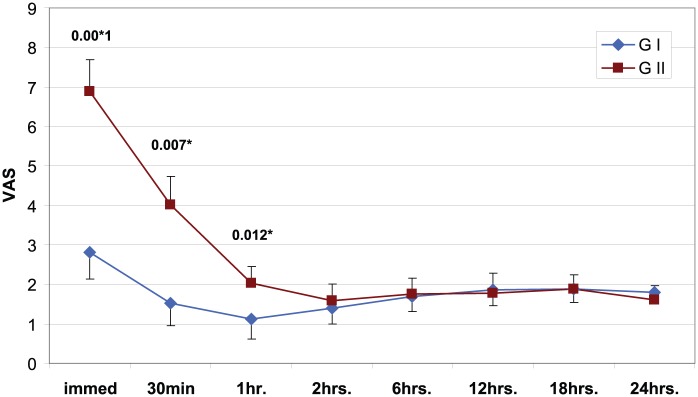
Results: Visual Analogue Scale (VAS) score was significantly lower in group I immediately, 30 minutes and 1 hour postoperatively. Time to first ambulation, return of intestinal sounds and hospital stay were shorter in group I than group II (p < 0.05); total morphine consumption was significantly lower in group I than group II (p < 0.05). Sedation score was significantly higher in group I immediately postoperatively, while at 30 minutes, 1, 2 and 6 hours postoperatively sedation scores were significantly higher in group II. Itching was significantly higher in group I.
Conclusion: The addition of IT morphine to a multimodal analgesic regimen after laparoscopic bariatric surgery was an effective and safe method that markedly reduced postoperative pain, systemic opioid consumption and length of hospital stay.
Keywords: Intrathecal morphine; laparoscopic bariatric surgery; multimodal analgesia; postoperative pain management.
Conflict of interest statement
Declaration of conflicting interest: The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Figures


References
-
- Joris JL, Hinque VL, Laurent PE, et al. Pulmonary function and pain after gastroplasty performed via laparotomy or laparoscopy in morbidly obese patients. Br J Anaesth 1998; 80(3): 283–288. - PubMed
-
- Ballantyne JC, Carr DB, deFerranti S, et al. The comparative effects of postoperative analgesic therapies on pulmonary outcome: cumulative meta-analyses of randomized, controlled trials. Anesth Analg 1998; 86(3): 598–612. - PubMed
-
- Escalante-Tattersfield T, Tucker O, Fajnwaks P, et al. Incidence of deep vein thrombosis in morbidly obese patients undergoing laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis 2008; 4(2): 126–130. - PubMed
-
- Kehlet H, Holte K. Effect of postoperative analgesia on surgical outcome. Br J Anaesth 2001; 87(1): 62–72. - PubMed
-
- Flancbaum L, Choban PS. Surgical implications of obesity. Annu Rev Med 1998; 49: 215–234. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources