

A morphologic study of the airway structure abnormalities in patients with asthma by high-resolution computed tomography
- PMID: 27867544
- PMCID: PMC5107441
- DOI: 10.21037/jtd.2016.09.36
A morphologic study of the airway structure abnormalities in patients with asthma by high-resolution computed tomography
Abstract
Background: Airway structure changes, termed as airway remodeling, are common in asthma patients due to chronic inflammation, which can be assessed by high-resolution computed tomography (HRCT). Considering the controversial conclusions in the correlation of morphologic abnormalities with clinical feature and outcome, we aimed to further specify and evaluate the structural abnormalities of Chinese asthmatics by HRCT.
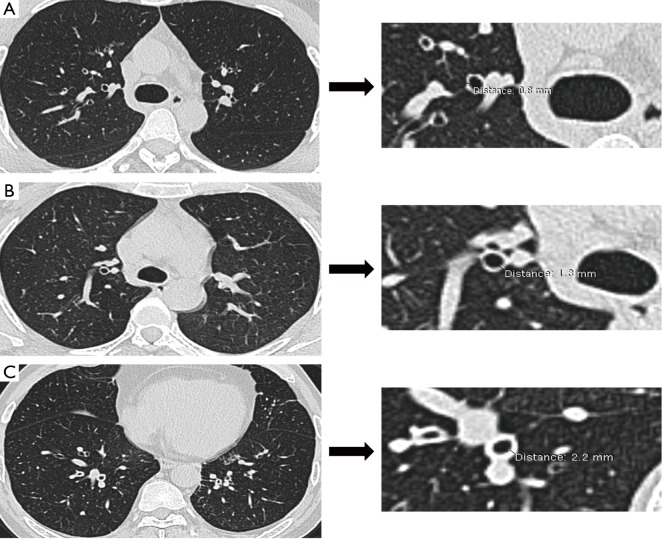
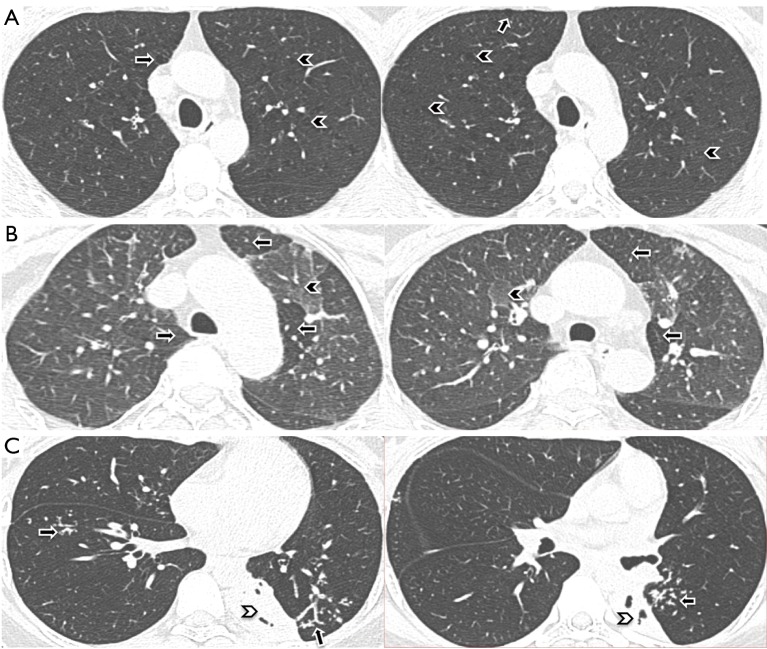
Methods: From August 2012 to February 2015, outpatients with asthma were recruited consecutively in the Asthma Center of West China Hospital, Sichuan University. Standard HRCT and pulmonary function test (PFT) were performed to collect information of bronchial wall thickening, bronchial dilatation, mucus impaction, emphysema, mosaic perfusion, atelectasis, and spirometric parameters. We reported the incidence of each structural abnormality in HRCT and compared it among different asthmatic severities.
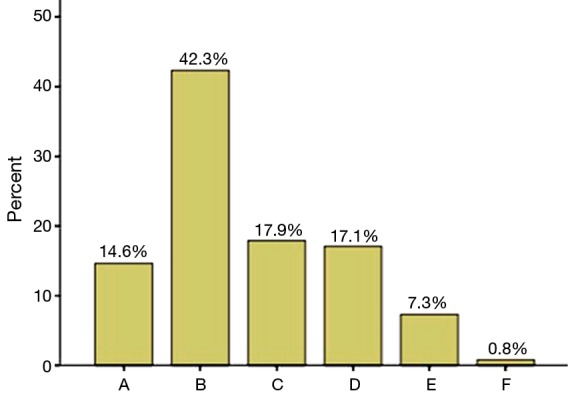
Results: A total of 123 asthmatics were enrolled, among which 84 (68.3%) were female and 39 (31.7%) were male. At least one structural abnormality was detected by HRCT in 85.4% asthmatics, and the incidence of bronchial wall thickening, bronchial dilatation, mucus impaction, emphysema, mosaic perfusion, and atelectasis was 57.7%, 51.2%, 22%, 24.4%, 5.7% and 1.6%, respectively. The incidences of bronchial wall thickening, bronchial dilation and emphysema were significantly increased by asthma severity (P<0.05), while incidences of mucus impaction (26/27, 96.30%), mosaic perfusion (6/7, 85.71%) and atelectasis (2/2, 100%) were mainly found in severe asthma. We found a longer asthma history (28.13±18.55 years, P<0.001, P=0.003), older age (51.30±10.70 years, P=0.022, P=0.006) and lower predicted percentage of forced expiratory volume in one second (FEV1%) (41.97±15.19, P<0.001, P<0.001) and ratio of forced expiratory volume to forced vital capacity (FEV1/FVC) (48.01±9.55, P<0.001, P<0.001) in patients with severe bronchial dilation compared with those in none and mild bronchial dilation. A negative correlation was also found between the extent of bronchial dilation and FEV1% as well as FEV1/FVC (r=-0.359, P=0.004; r=-0.266, P=0.035, respectively).
Conclusions: The incidences of structural abnormalities detected by HRCT are fairly high in Chinese asthma populations, especially the bronchial wall thickening and bronchial dilation, which are significantly increased in severe asthma, and are potential risk factors of pulmonary function decline in asthmatics.
Keywords: Bronchial asthma; airway remodeling; bronchiectasis; high-resolution computed tomography (HRCT).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures

References
-
- Global Strategy for Asthma Management and Prevention. Global Initiative for Asthma (GINA), 2014. Available online: www.ginasthma.org, accessed on August 12, 2014.
-
- Ge JB, Xu YJ. Internal Medicine. Beijing: People’s Medical Publishing House, 2013.
LinkOut - more resources
Full Text Sources
Other Literature Sources