

Analysis of risk factors for and the prognosis of postoperative acute respiratory distress syndrome in patients with Stanford type A aortic dissection
- PMID: 27867562
- PMCID: PMC5107558
- DOI: 10.21037/jtd.2016.10.10
Analysis of risk factors for and the prognosis of postoperative acute respiratory distress syndrome in patients with Stanford type A aortic dissection
Abstract
Background: To explore the risk factors for and the prognosis of postoperative acute respiratory distress syndrome (ARDS) in patients with Stanford type A aortic dissection (AD).
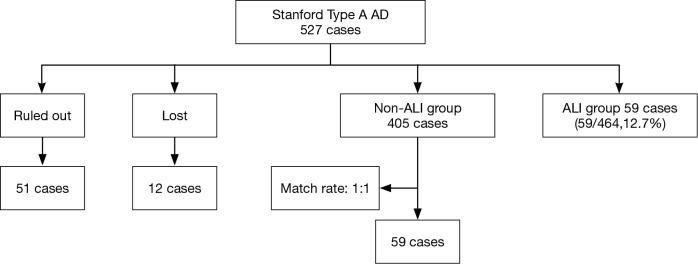
Methods: This retrospective nested case-control study included 527 Stanford type A AD patients who were divided into ARDS groups and non-ARDS groups. The clinical features of the groups were examined.
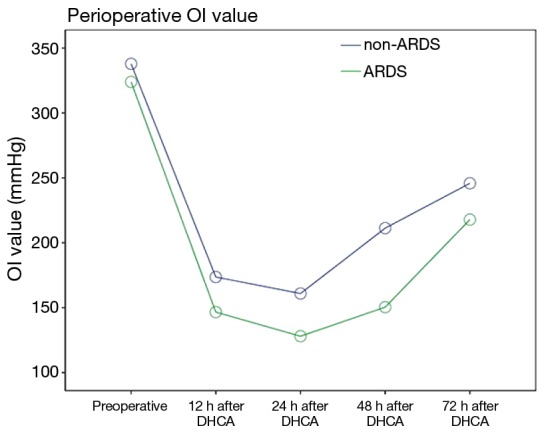
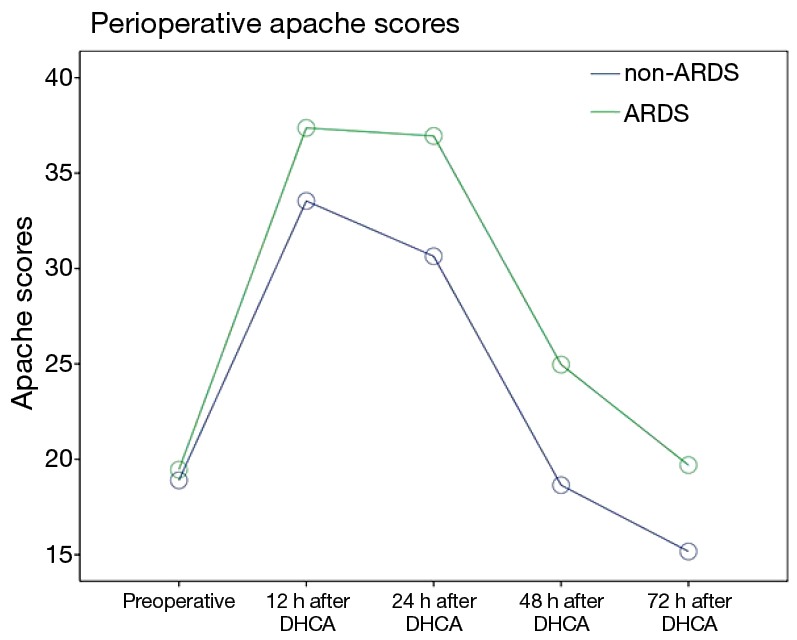
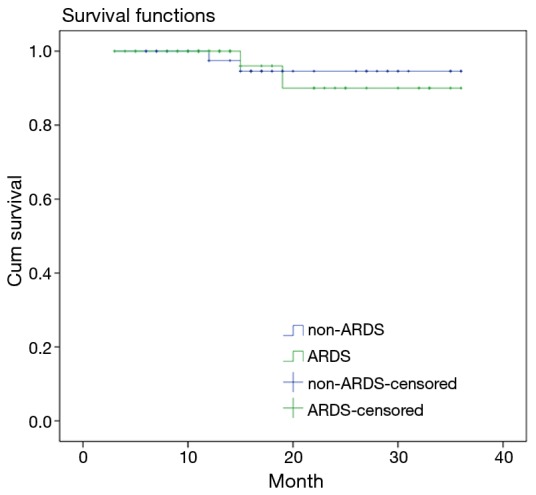
Results: The fifty-nine patients in the ARDS group exhibited extended durations of cardiopulmonary bypass (CPB) (P=0.004), deep hypothermic circulatory arrest (DHCA) (P=0.000), ventilator support (P=0.013) and intensive care unit (ICU) stay (P=0.045), higher hospital costs (P=0.000), larger perioperative transfusions volumes [red blood cells (RBC): P=0.002, platelets (PLT): P=0.040, fresh frozen plasma (FFP): P=0.001], more frequent pulmonary infection (P=0.018) and multiple organ dysfunction syndrome (MODS) (P=0.040) and a higher rate of in-hospital mortality (P=0.020). The ARDS group exhibited worse statuses in terms of oxygenation index (OI) values (P=0.000) and Apache II scores (P=0.000). DHCA [P=0.000, odds ratio (OR) =2.589] and perioperative transfusion (RBC: P=0.000, OR =2.573; PLT: P=0.027, OR =1.571; FFP: P=0.002, OR =1.929) were independent risk factors for postoperative ARDS. The survival rates and median survival times after discharge were similar between the two groups (P=0.843).
Conclusions: DHCA duration and perioperative transfusion volume were independent risk factors for postoperative ARDS which warrants greater attention by the cardiac surgeons.
Keywords: Respiratory distress syndrome; adult; aortic aneurysm; cardiopulmonary bypass; circulatory arrest; deep hypothermia induced.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Similar articles
-
The risk factors for postoperative acute respiratory distress syndrome in Stanford type a acute aortic dissection patients.Am J Transl Res. 2021 Jun 15;13(6):7318-7326. eCollection 2021. Am J Transl Res. 2021. PMID: 34306500 Free PMC article.
-
Aprotinin, blood loss, and renal dysfunction in deep hypothermic circulatory arrest.Circulation. 2001 Sep 18;104(12 Suppl 1):I276-81. doi: 10.1161/hc37t1.094702. Circulation. 2001. PMID: 11568069
-
Deep hypothermic circulatory arrest versus non-deep hypothermic beating heart strategy in descending thoracic or thoracoabdominal aortic surgery.Eur J Cardiothorac Surg. 2014 Oct;46(4):678-84. doi: 10.1093/ejcts/ezu053. Epub 2014 Feb 26. Eur J Cardiothorac Surg. 2014. PMID: 24578408
-
[1/1 plasma to red blood cell ratio: an evidence-based practice?].Ann Fr Anesth Reanim. 2011 May;30(5):421-8. doi: 10.1016/j.annfar.2011.02.015. Epub 2011 Apr 29. Ann Fr Anesth Reanim. 2011. PMID: 21531112 Review. French.
-
Acute respiratory distress syndrome after cardiac surgery.J Thorac Dis. 2016 Oct;8(10):E1177-E1186. doi: 10.21037/jtd.2016.10.74. J Thorac Dis. 2016. PMID: 27867583 Free PMC article. Review.
Cited by
-
Oxygenation impairment in patients with acute aortic dissection is associated with disorders of coagulation and fibrinolysis: a prospective observational study.J Thorac Dis. 2019 Apr;11(4):1190-1201. doi: 10.21037/jtd.2019.04.32. J Thorac Dis. 2019. PMID: 31179061 Free PMC article.
-
Patient functionality and walking speed after discharge from the intensive care unit.Rev Bras Ter Intensiva. 2019 Oct-Dec;31(4):529-535. doi: 10.5935/0103-507X.20190066. Rev Bras Ter Intensiva. 2019. PMID: 31967228 Free PMC article.
-
Case Report: The role of nitric oxide inhalation and prone positioning ventilation in oxygen improvement in patients with refractory hypoxemia following acute type A aortic dissection surgery: two cases report and literature review.Front Cardiovasc Med. 2025 Jul 4;12:1627953. doi: 10.3389/fcvm.2025.1627953. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40687562 Free PMC article.
-
Perioperative oxygenation impairment related to type a aortic dissection.Perfusion. 2025 Jan;40(1):49-60. doi: 10.1177/02676591231224997. Epub 2024 Jan 4. Perfusion. 2025. PMID: 38174389 Free PMC article. Review.
-
Perioperative Risk Factors for Post-operative Pneumonia after Type A Acute Aortic Dissection Surgery.Curr Med Sci. 2023 Feb;43(1):69-79. doi: 10.1007/s11596-022-2659-4. Epub 2022 Nov 5. Curr Med Sci. 2023. PMID: 36334171
References
LinkOut - more resources
Full Text Sources
Other Literature Sources