

Optimal Treatment Decision for Brain Metastases of Unknown Primary Origin: The Role and Timing of Radiosurgery
- PMID: 27867920
- PMCID: PMC5114180
- DOI: 10.14791/btrt.2016.4.2.107
Optimal Treatment Decision for Brain Metastases of Unknown Primary Origin: The Role and Timing of Radiosurgery
Abstract
Background: Up to 15% of all patients with brain metastases have no clearly detected primary site despite intensive evaluation, and this incidence has decreased with the use of improved imaging technology. Radiosurgery has been evaluated as one of the treatment modality for patients with limited brain metastases. In this study, we evaluated the effectiveness of radiosurgery for brain metastases from unknown primary tumors.
Methods: We retrospectively evaluated 540 patients who underwent gamma knife radiosurgery (GKRS) for brain metastases radiologically diagnosed between August 1992 and September 2007 in our institution. First, the brain metastases were grouped into metachronous, synchronous, and precocious presentations according to the timing of diagnosis of the brain metastases. Then, synchronous and precocious brain metastases were further grouped into 1) unknown primary; 2) delayed known primary; and 3) synchronous metastases according to the timing of diagnosis of the primary origin. We analyzed the survival time and time to new brain metastasis in each group.
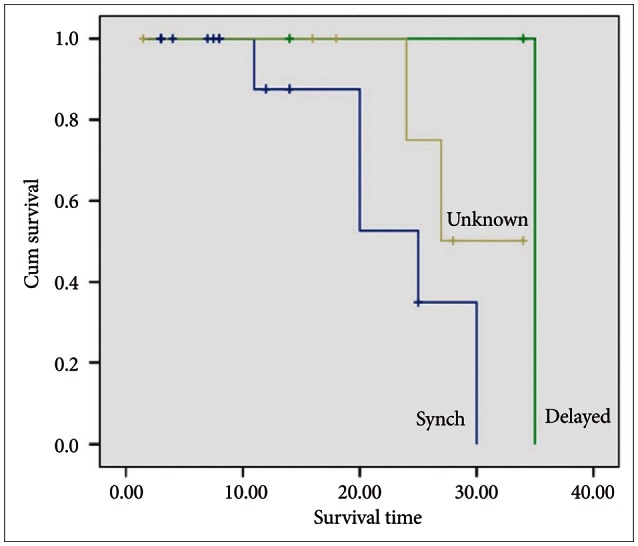
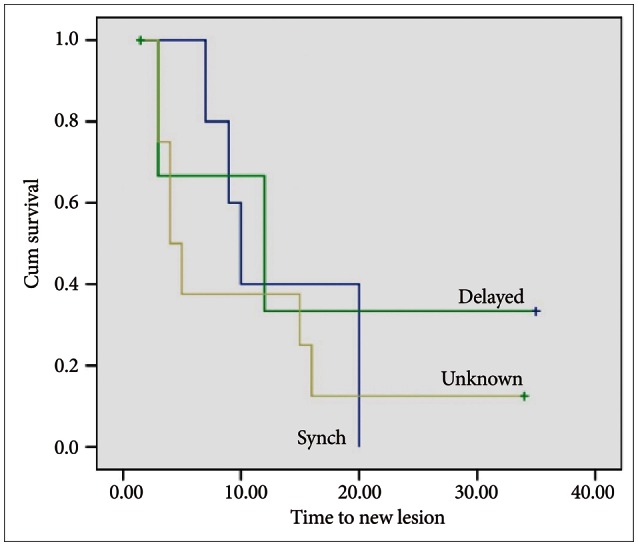
Results: Of the 540 patients, 29 (5.4%) presented precocious or synchronous metastases (34 GKRS procedures for 174 lesions). The primary tumor was not found even after intensive and repeated systemic evaluation in 10 patients (unknown primary, 34.5%); found after 8 months in 3 patients (delayed known primary, 1.2%); and diagnosed at the same time as the brain metastases in 16 patients (synchronous metastasis, 55.2%). No statistically significant differences in survival time and time to new brain metastasis were found among the three groups.
Conclusion: Identification of a primary tumor before GKRS did not affect the patient outcomes. If other possible differential diagnoses were completely excluded, early GKRS can be an effective treatment option for brain metastases from unknown primary tumor.
Keywords: Neoplasm metastasis; Neoplasms, Unknown primary; Radiosurgery.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Patchell RA. The management of brain metastases. Cancer Treat Rev. 2003;29:533–540. - PubMed
-
- Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet. 2004;363:1665–1672. - PubMed
-
- Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA. 2006;295:2483–2491. - PubMed
-
- Chang EL, Wefel JS, Hess KR, et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: a randomised controlled trial. Lancet Oncol. 2009;10:1037–1044. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
