

The Impact of Radiation Treatment Time on Survival in Patients With Head and Neck Cancer
- PMID: 27869097
- PMCID: PMC5147736
- DOI: 10.1016/j.ijrobp.2016.08.046
The Impact of Radiation Treatment Time on Survival in Patients With Head and Neck Cancer
Abstract
Purpose: To assess the impact of radiation treatment time (RTT) in head and neck cancers on overall survival (OS) in the era of chemoradiation.
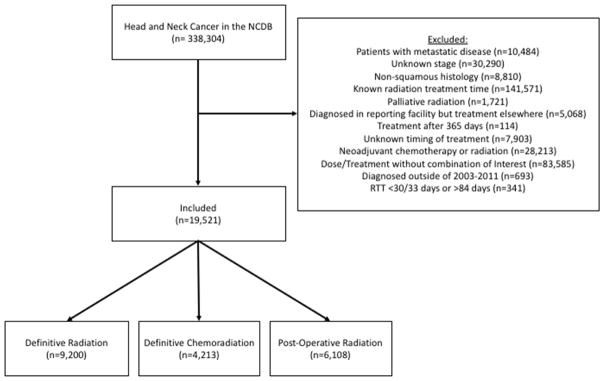
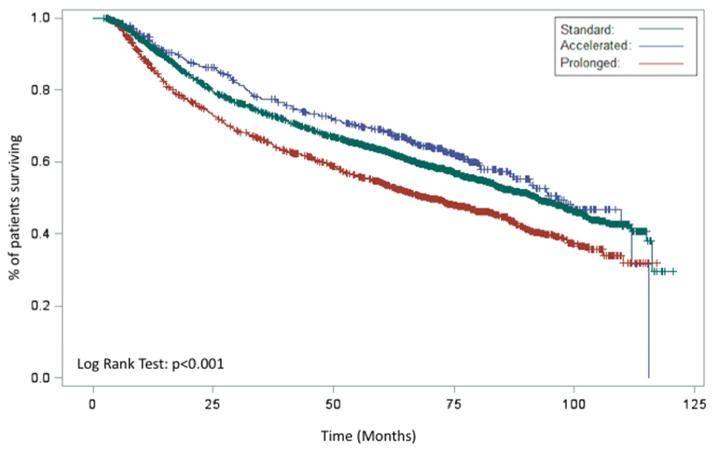
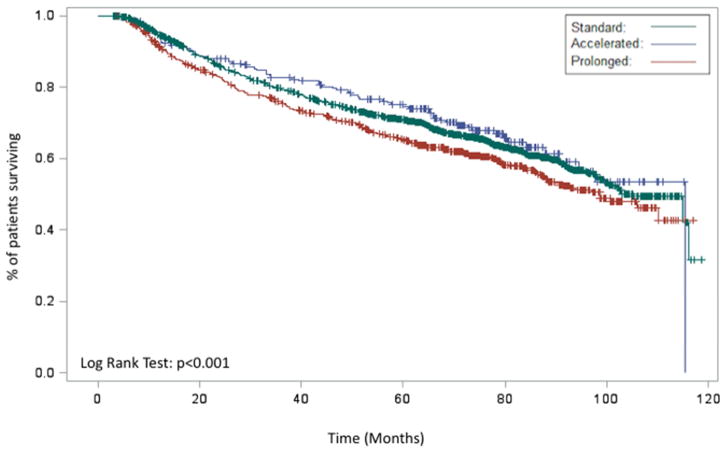
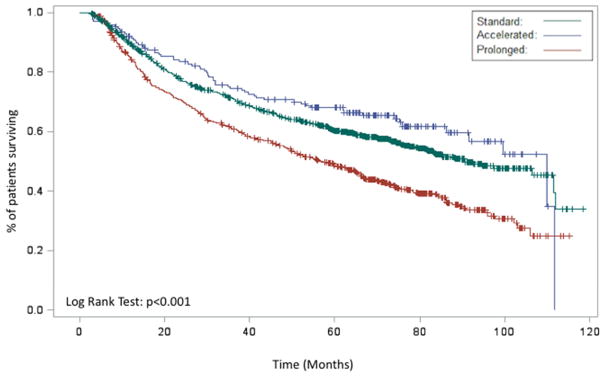
Methods and materials: Patients with diagnoses of tongue, hypopharynx, larynx, oropharynx, or tonsil cancer were identified by use of the National Cancer Database. RTT was defined as date of first radiation treatment to date of last radiation treatment. In the definitive setting, prolonged RTT was defined as >56 days, accelerated RTT was defined as <47 days, and standard RTT was defined as 47 to 56 days. In the postoperative setting, prolonged RTT was defined as >49 days, accelerated RTT was defined as <40 days, and standard RTT was defined as 40 to 49 days. We used χ2 tests to identify predictors of RTT. The Kaplan-Meier method was used to compare OS among groups. Cox proportional hazards model was used for OS analysis in patients with known comorbidity status.
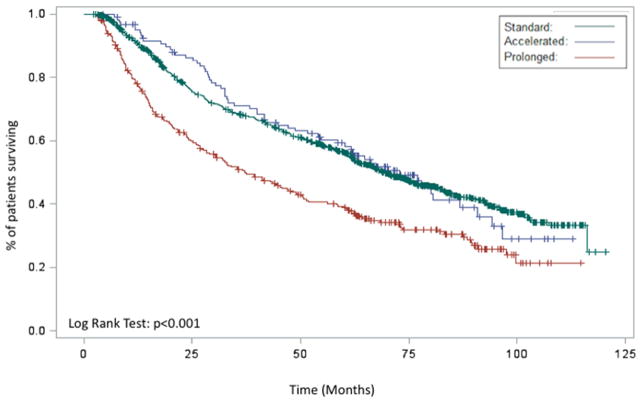
Results: 19,531 patients were included; 12,987 (67%) had a standard RTT, 4,369 (34%) had an accelerated RTT, and 2,165 (11%) had a prolonged RTT. On multivariable analysis, accelerated RTT (hazard ratio [HR] 0.84; 95% confidence interval [CI] 0.73-0.97) was associated with an improved OS, and prolonged RTT (HR 1.25; 95% CI 1.14-1.37) was associated with a worse OS relative to standard RTT. When the 9,200 (47%) patients receiving definitive concurrent chemoradiation were examined, prolonged RTT (HR 1.29; 95% CI 1.11-1.50) was associated with a worse OS relative to standard RTT, whereas there was no significant association between accelerated RTT and OS (HR 0.76; 95% CI 0.57-1.01).
Conclusion: Prolonged RTT is associated with worse OS in patients receiving radiation therapy for head and neck cancer, even in the setting of chemoradiation. Expeditious completion of radiation should continue to be a quality metric for the management of head and neck malignancies.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
None
Figures
References
-
- Fyles A, Keane TJ, Barton M, Simm J. The effect of treatment duration in the local control of cervix cancer. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology. 1992;25(4):273–279. - PubMed
-
- Chen M, Jiang GL, Fu XL, et al. The impact of overall treatment time on outcomes in radiation therapy for non-small cell lung cancer. Lung Cancer. 2000;28(1):11–19. - PubMed
-
- Perez CA, Grigsby PW, Castro-Vita H, Lockett MA. Carcinoma of the uterine cervix. I. Impact of prolongation of overall treatment time and timing of brachytherapy on outcome of radiation therapy. International journal of radiation oncology, biology, physics. 1995;32(5):1275–1288. - PubMed
-
- Kim JJ, Tannock IF. Repopulation of cancer cells during therapy: An important cause of treatment failure. Nature reviews Cancer. 2005;5(7):516–525. - PubMed
-
- Withers HR, Taylor JM, Maciejewski B. The hazard of accelerated tumor clonogen repopulation during radiotherapy. Acta oncologica. 1988;27(2):131–146. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
