

The Selective Serotonin Reuptake Inhibitor Fluoxetine Directly Inhibits Osteoblast Differentiation and Mineralization During Fracture Healing in Mice
- PMID: 27869327
- PMCID: PMC5395314
- DOI: 10.1002/jbmr.3045
The Selective Serotonin Reuptake Inhibitor Fluoxetine Directly Inhibits Osteoblast Differentiation and Mineralization During Fracture Healing in Mice
Abstract
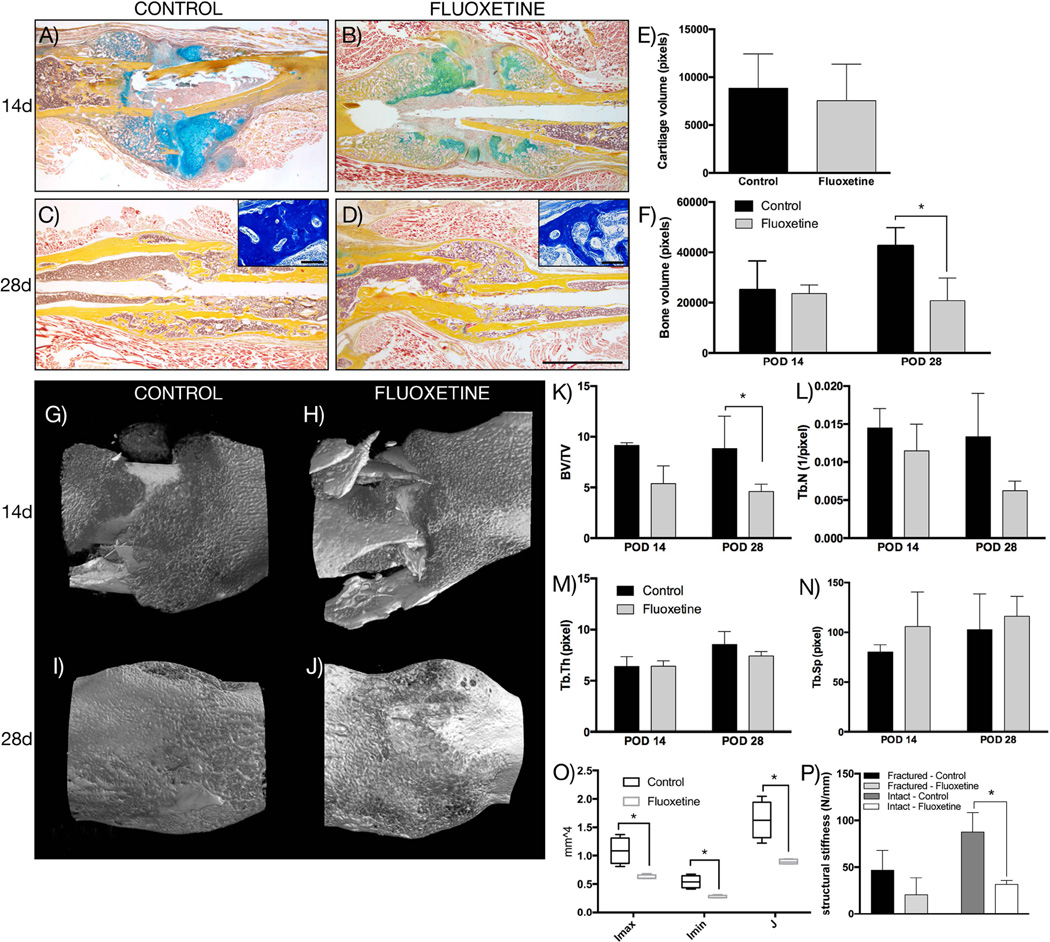
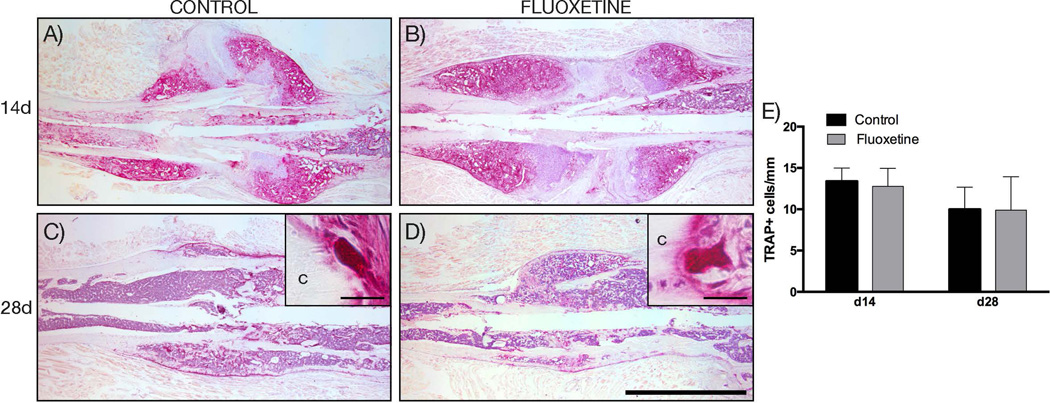
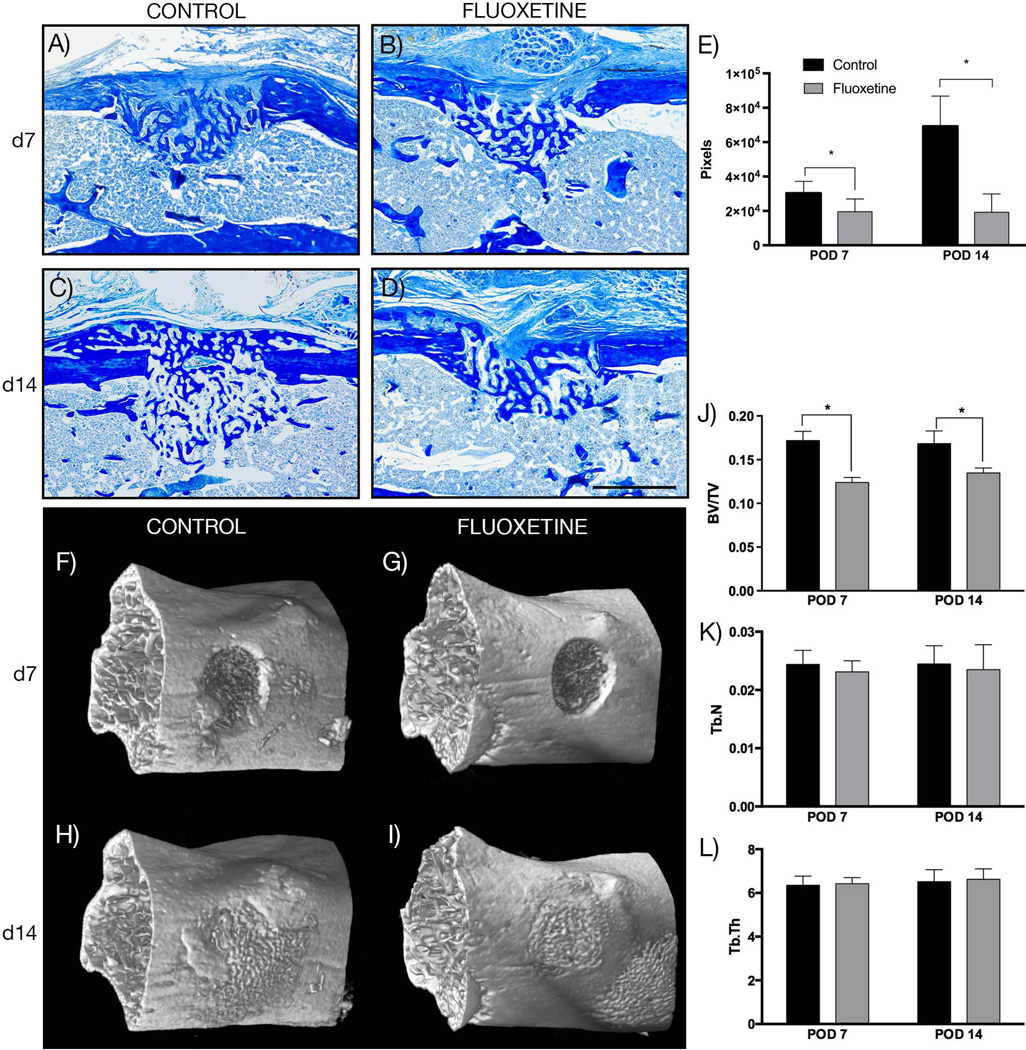
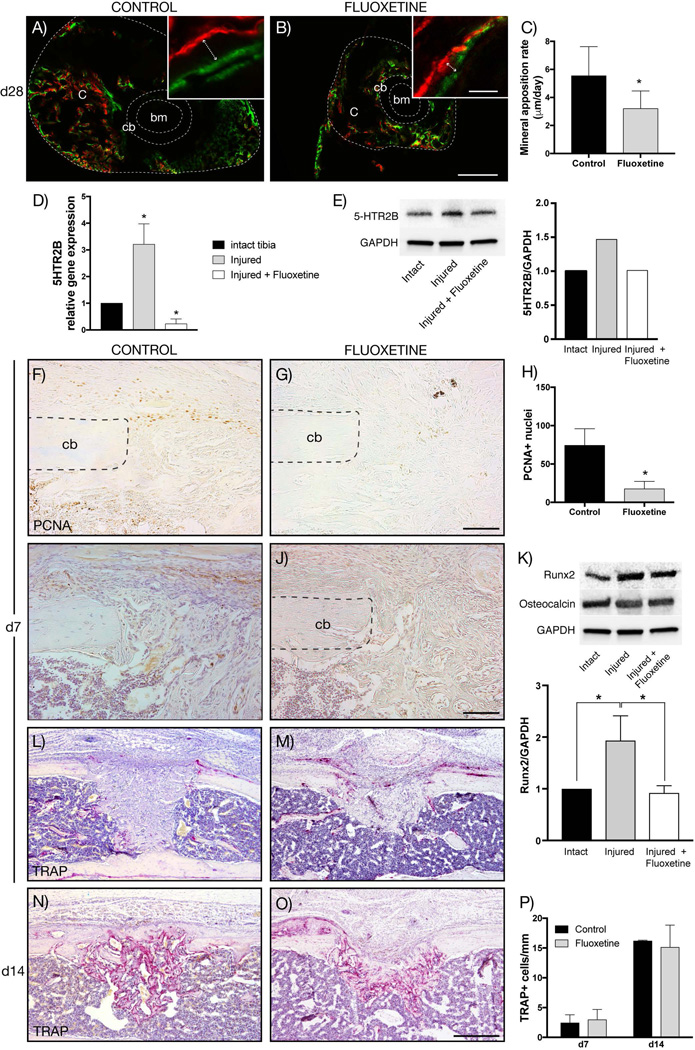
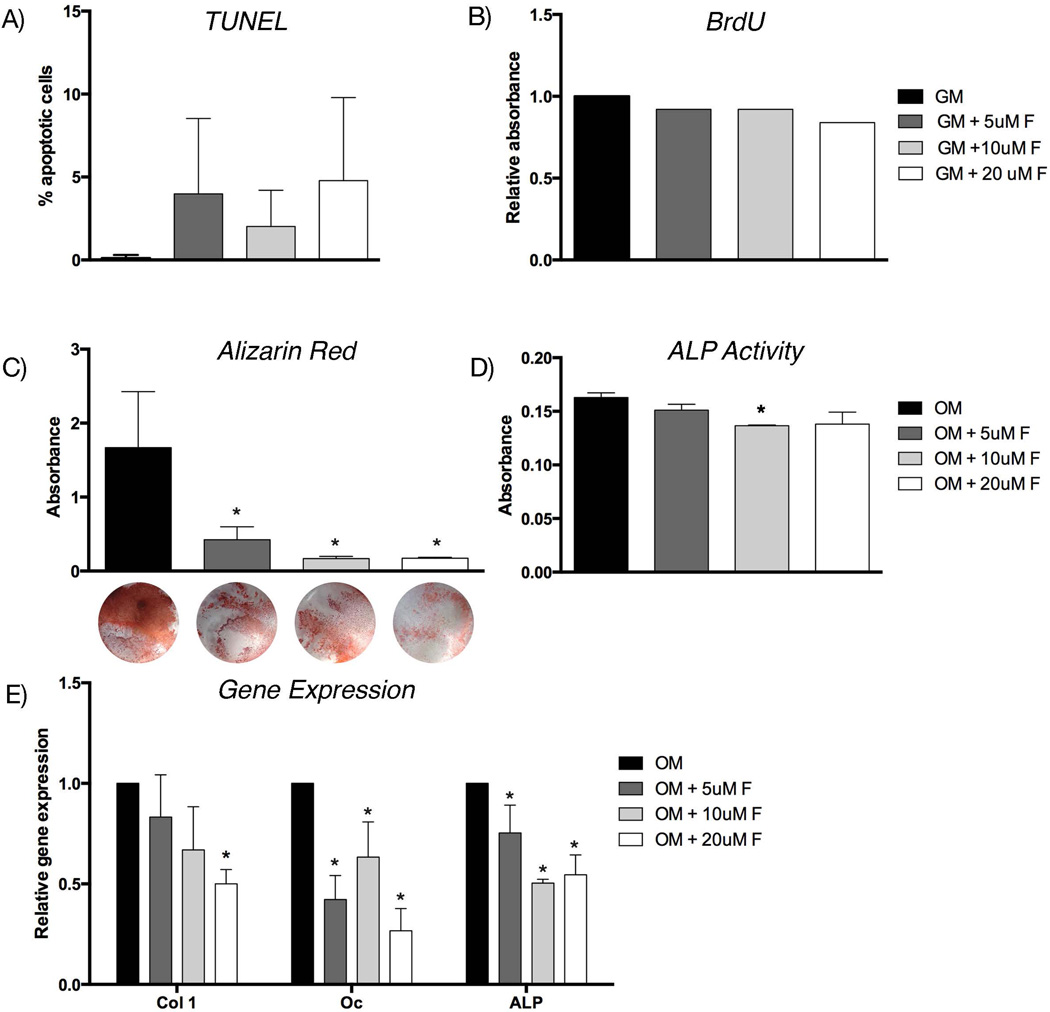
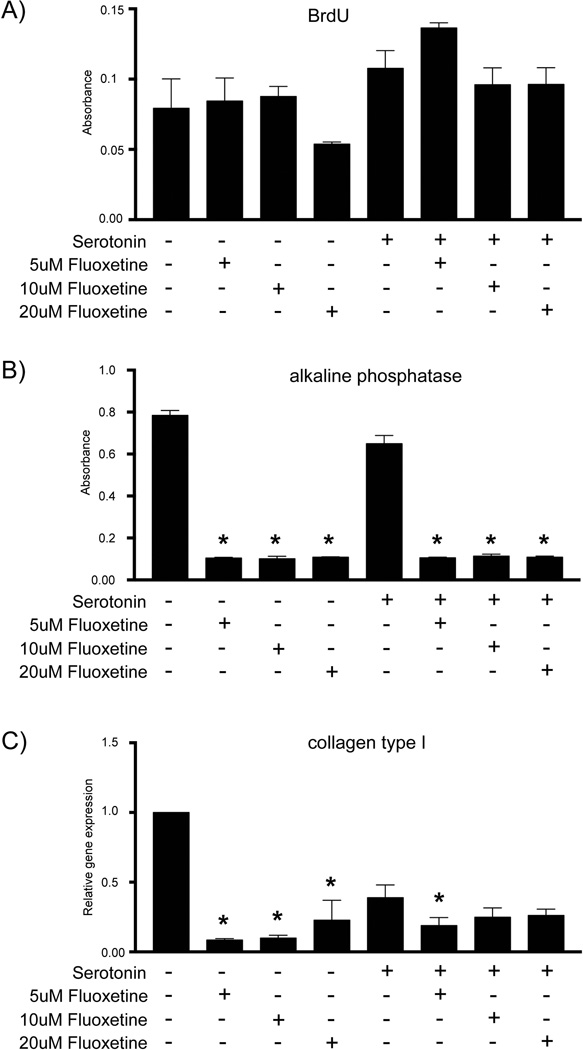
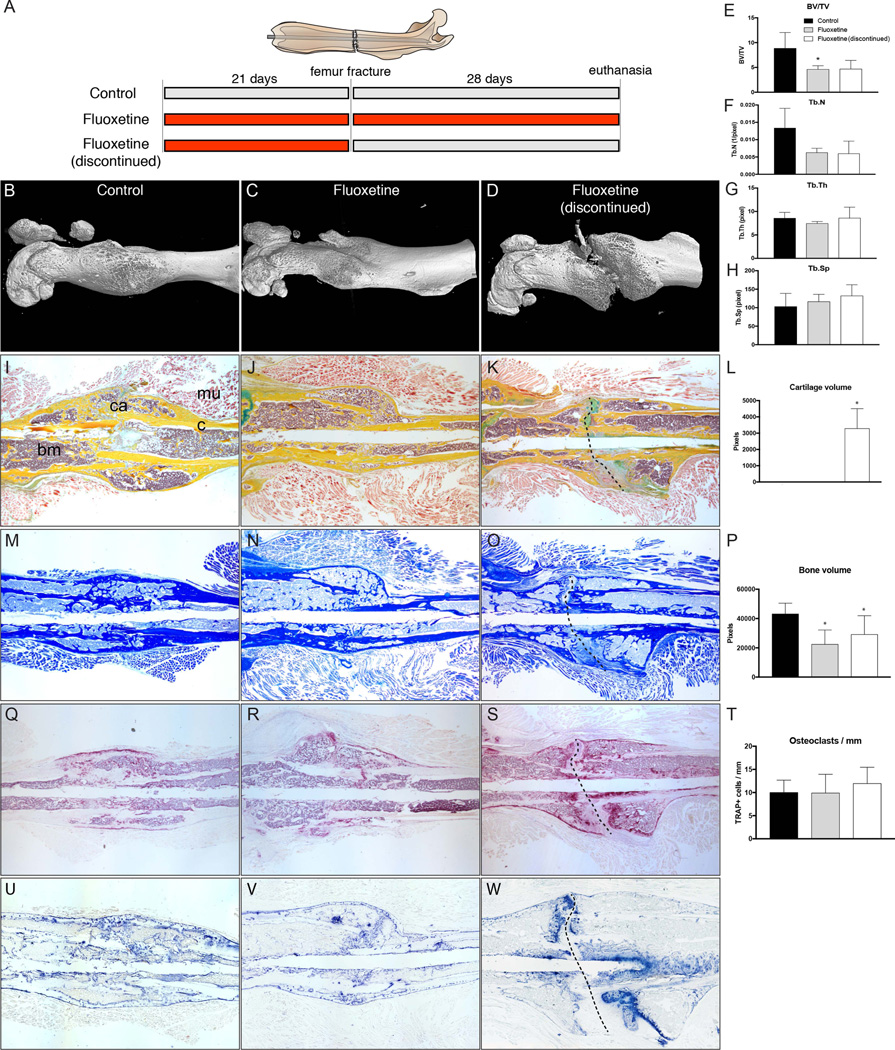
Chronic use of selective serotonin reuptake inhibitors (SSRIs) for the treatment of depression has been linked to osteoporosis. In this study, we investigated the effect of chronic SSRI use on fracture healing in two murine models of bone regeneration. First, we performed a comprehensive analysis of endochondral bone healing in a femur fracture model. C57/BL6 mice treated with fluoxetine, the most commonly prescribed SSRI, developed a normal cartilaginous soft-callus at 14 days after fracture and demonstrated a significantly smaller and biomechanically weaker bony hard-callus at 28 days. In order to further dissect the mechanism that resulted in a smaller bony regenerate, we used an intramembranous model of bone healing and revealed that fluoxetine treatment resulted in a significantly smaller bony callus at 7 and 14 days postinjury. In order to test whether the smaller bony regenerate following fluoxetine treatment was caused by an inhibition of osteogenic differentiation and/or mineralization, we employed in vitro experiments, which established that fluoxetine treatment decreases osteogenic differentiation and mineralization and that this effect is serotonin-independent. Finally, in a translational approach, we tested whether cessation of the medication would result in restoration of the regenerative potential. However, histologic and μCT analysis revealed non-union formation in these animals with fibrous tissue interposition within the callus. In conclusion, fluoxetine exerts a direct, inhibitory effect on osteoblast differentiation and mineralization, shown in two disparate murine models of bone repair. Discontinuation of the drug did not result in restoration of the healing potential, but rather led to complete arrest of the repair process. Besides the well-established effect of SSRIs on bone homeostasis, our study provides strong evidence that fluoxetine use negatively impacts fracture healing. © 2017 American Society for Bone and Mineral Research.
Keywords: BONE; DEPRESSION; OSTEOBLAST; OSTEOPOROSIS; OSTEOPROGENITOR CELL.
© 2017 American Society for Bone and Mineral Research.
Figures
Similar articles
-
Propranolol Reverses Impaired Fracture Healing Response Observed With Selective Serotonin Reuptake Inhibitor Treatment.J Bone Miner Res. 2020 May;35(5):932-941. doi: 10.1002/jbmr.3950. Epub 2020 Jan 10. J Bone Miner Res. 2020. PMID: 31881108 Free PMC article.
-
Methylglyoxal compromises callus mineralization and impairs fracture healing through suppression of osteoblast terminal differentiation.Biochem Biophys Res Commun. 2025 Feb 2;747:151312. doi: 10.1016/j.bbrc.2025.151312. Epub 2025 Jan 9. Biochem Biophys Res Commun. 2025. PMID: 39799866
-
Temporary inhibition of the plasminogen activator inhibits periosteal chondrogenesis and promotes periosteal osteogenesis during appendicular bone fracture healing.Bone. 2018 Jul;112:97-106. doi: 10.1016/j.bone.2018.04.016. Epub 2018 Apr 19. Bone. 2018. PMID: 29680264 Free PMC article.
-
Fracture healing in osteoporotic bone.Injury. 2016 Jun;47 Suppl 2:S21-6. doi: 10.1016/S0020-1383(16)47004-X. Injury. 2016. PMID: 27338222 Review.
-
Effect of osteoporosis medications on fracture healing.Osteoporos Int. 2016 Mar;27(3):861-871. doi: 10.1007/s00198-015-3331-7. Epub 2015 Sep 29. Osteoporos Int. 2016. PMID: 26419471 Review.
Cited by
-
Evaluation of the increased risk of spine fracture in patients with mood disorder compared with matched controls: a longitudinal follow-up study using a national sample cohort in Korea.BMJ Open. 2019 Nov 28;9(11):e027581. doi: 10.1136/bmjopen-2018-027581. BMJ Open. 2019. PMID: 31784429 Free PMC article.
-
Serotonin Reuptake Inhibitor Increases Pseudarthrosis Rates in Anterior Cervical Discectomy and Fusions.Asian Spine J. 2023 Apr;17(2):304-312. doi: 10.31616/asj.2022.0065. Epub 2023 Jan 10. Asian Spine J. 2023. PMID: 36625020 Free PMC article.
-
[Influence of frequently prescribed drugs on bone healing].Unfallchirurg. 2019 Jul;122(7):500-505. doi: 10.1007/s00113-019-0670-4. Unfallchirurg. 2019. PMID: 31214745 Review. German.
-
Hox gene expression determines cell fate of adult periosteal stem/progenitor cells.Sci Rep. 2019 Mar 25;9(1):5043. doi: 10.1038/s41598-019-41639-7. Sci Rep. 2019. PMID: 30911091 Free PMC article.
-
The Effect of Antidepressants on Mesenchymal Stem Cell Differentiation.J Bone Metab. 2018 Feb;25(1):43-51. doi: 10.11005/jbm.2018.25.1.43. Epub 2018 Feb 28. J Bone Metab. 2018. PMID: 29564305 Free PMC article.
References
-
- Feuer AJ, Demmer RT, Thai A, Vogiatzi MG. Use of selective serotonin reuptake inhibitors and bone mass in adolescents: an NHANES study. Bone. 2015;78:28–33. - PubMed
-
- Wysowski DK, Governale LA, Swann J. Trends in outpatient prescription drug use and related costs in the US: 1998–2003. Pharmacoeconomics. 2006;24(3):233–236. - PubMed
-
- Rizzoli R, Cooper C, Reginster J-Y, et al. Antidepressant medications and osteoporosis. Bone. 2012;51(3):606–613. - PubMed
-
- Richter T, Paluch Z, Alusik S. The non-antidepressant effects of citalopram: a clinician’s perspective. Neuro Endocrinol Lett. 2014;35(1):7–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
