

Management strategies in Lynch syndrome and familial adenomatous polyposis: a national healthcare survey in Japan
- PMID: 27870147
- PMCID: PMC5329156
- DOI: 10.1111/cas.13123
Management strategies in Lynch syndrome and familial adenomatous polyposis: a national healthcare survey in Japan
Erratum in
-
Correction.Cancer Sci. 2017 Apr;108(4):804. doi: 10.1111/cas.13258. Cancer Sci. 2017. PMID: 28447392 Free PMC article. No abstract available.
Abstract
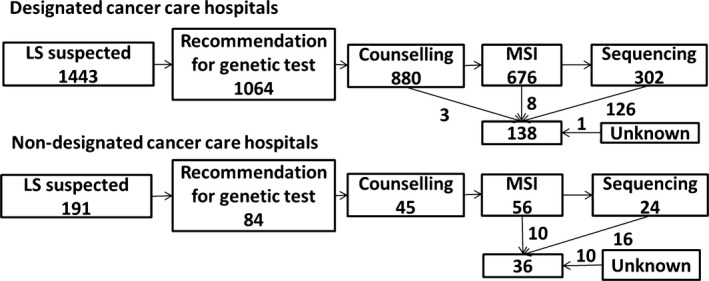
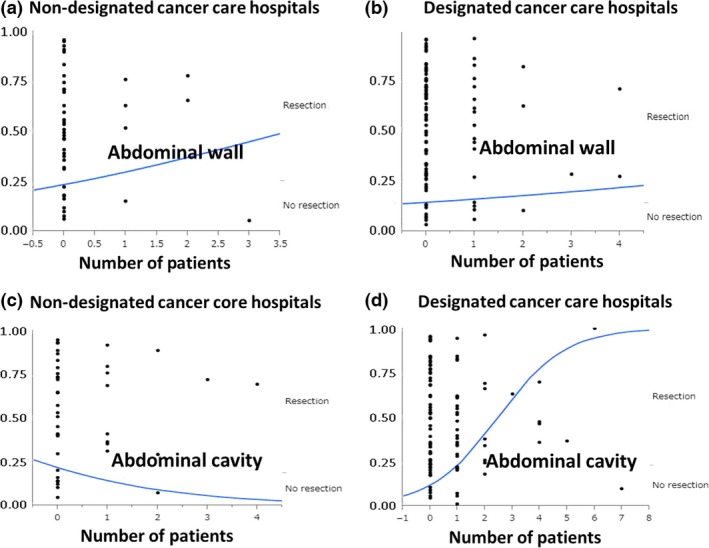
Lynch syndrome (LS) and familial adenomatous polyposis (FAP) are major sources of hereditary colorectal cancer (CRC) and are associated with other malignancies. There is some heterogeneity in management strategies in Japan. We undertook a survey of management of hereditary CRC in hospitals that are members of the Japan Society of Colorectal Cancer Research. One hundred and ninety departments responded, of which 127 were from designated cancer care hospitals (DCCHs) according to the Japanese government. There were 25 488 operations for CRC in these departments in 2015. The DCCHs performed better with regard to usage of Japan Society of Colorectal Cancer Research guidelines, referring new CRC patients for LS screening, and having in-house genetic counselors and knowledge of treatment for LS. There were 174 patients diagnosed with LS and 602 undergoing follow-up in 2011-2015, which is fewer than the number expected from CRC operations in 2015. These numbers were not affected by whether the institution was a DCCH. Universal screening for LS was carried out in 8% of the departments. In contrast, 541 patients were diagnosed with FAP and 273 received preventive proctocolectomy/colectomy in 2011-2015. The DCCH departments undertook more surgery than non-DCCH departments, although most of the management, including surgical procedures and use of non-steroidal anti-inflammatory drugs, was similar. Management of desmoid tumor in the abdominal cavity differed according to the number of patients treated. In conclusion, there was heterogeneity in management of LS but not FAP. Most patients with LS may be overlooked and universal screening for LS is not common in Japan.
Keywords: Disease management; Japanese; Lynch syndrome; familial adenomatous polyposis; screening.
© 2016 The Authors. Cancer Science published by John Wiley & Sons Australia, Ltd on behalf of Japanese Cancer Association.
Figures
Similar articles
-
Curative and Prophylactic Surgery of Young-onset Colorectal Cancer in Inherited Syndromes: A 15-Year Monocentric Retrospective Experience.Anticancer Res. 2019 Jun;39(6):3131-3136. doi: 10.21873/anticanres.13449. Anticancer Res. 2019. PMID: 31177158
-
The treatment of desmoid tumors associated with familial adenomatous polyposis: the results of a Japanese multicenter observational study.Surg Today. 2017 Oct;47(10):1259-1267. doi: 10.1007/s00595-017-1500-3. Epub 2017 Mar 1. Surg Today. 2017. PMID: 28251376
-
Role of surgery in familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer (Lynch syndrome).Surg Oncol Clin N Am. 2009 Oct;18(4):705-15. doi: 10.1016/j.soc.2009.07.006. Surg Oncol Clin N Am. 2009. PMID: 19793576 Review.
-
[Diagnosis and management of hereditary colorectal cancer according to the JSCCR Guidelines 2012 for the Clinical Practice of Hereditary Colorectal Cancer].Nihon Rinsho. 2014 Jan;72(1):143-9. Nihon Rinsho. 2014. PMID: 24597363 Review. Japanese.
-
[Current management status of hereditary colorectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Jun 25;25(6):546-551. doi: 10.3760/cma.j.cn441530-20211111-00457. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35754221 Chinese.
Cited by
-
Lynch Syndrome-Associated Variants and Cancer Rates in an Ancestrally Diverse Biobank.JCO Precis Oncol. 2020 Nov 23;4:PO.20.00290. doi: 10.1200/PO.20.00290. eCollection 2020. JCO Precis Oncol. 2020. PMID: 33283134 Free PMC article.
-
Evaluation of appropriate follow-up after curative surgery for patients with colorectal cancer using time to recurrence and survival after recurrence: a retrospective multicenter study.Oncotarget. 2018 May 22;9(39):25474-25490. doi: 10.18632/oncotarget.25312. eCollection 2018 May 22. Oncotarget. 2018. PMID: 29876002 Free PMC article.
-
Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2020 for the Clinical Practice of Hereditary Colorectal Cancer.Int J Clin Oncol. 2021 Aug;26(8):1353-1419. doi: 10.1007/s10147-021-01881-4. Epub 2021 Jun 29. Int J Clin Oncol. 2021. PMID: 34185173 Free PMC article.
-
Characteristics of Cancer in Subjects Carrying Lynch Syndrome-Associated Gene Variants in Taiwanese Population: A Hospital-Based Study in Taiwan.Cancers (Basel). 2024 Oct 31;16(21):3682. doi: 10.3390/cancers16213682. Cancers (Basel). 2024. PMID: 39518119 Free PMC article.
-
Long-term clinical outcomes and follow-up status in Japanese patients with familial adenomatous polyposis after radical surgery: a descriptive, retrospective cohort study from a single institute.Int J Colorectal Dis. 2020 Apr;35(4):675-684. doi: 10.1007/s00384-020-03524-y. Epub 2020 Feb 7. Int J Colorectal Dis. 2020. PMID: 32034491
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin 2015; 65: 5–29. - PubMed
-
- Arnold M, Sierra MS, Laversanne M et al Global patterns and trends in colorectal cancer incidence and mortality. Gut 2016. doi:10.1136/gutjnl‐2015‐310912.x. - DOI - PubMed
-
- Stoffel EM, Mangu PB, Gruber SB et al Hereditary colorectal cancer syndromes: American Society of Clinical Oncology clinical practice guideline endorsement of the familial risk‐colorectal cancer: European Society for Medical Oncology clinical practice guidelines. J Clin Oncol 2015; 33: 209–17. - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
