

High-Dose Chemotherapy and Autologous Peripheral-Blood Stem-Cell Transplantation for Relapsed Metastatic Germ Cell Tumors: The Indiana University Experience
- PMID: 27870561
- PMCID: PMC5455354
- DOI: 10.1200/JCO.2016.69.5395
High-Dose Chemotherapy and Autologous Peripheral-Blood Stem-Cell Transplantation for Relapsed Metastatic Germ Cell Tumors: The Indiana University Experience
Abstract
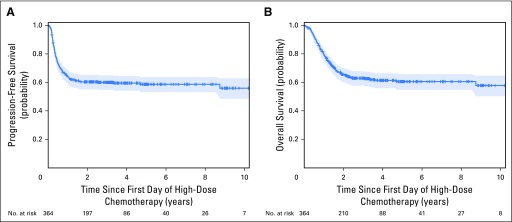
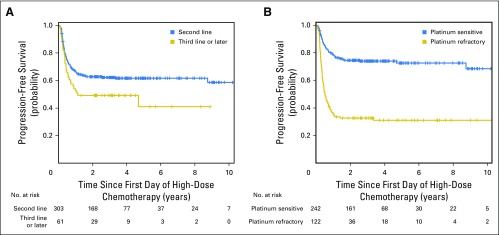
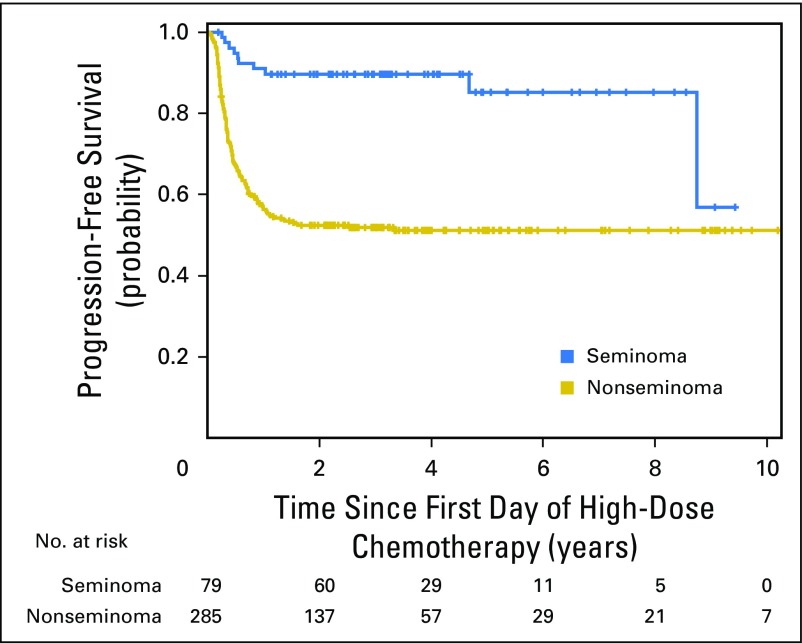
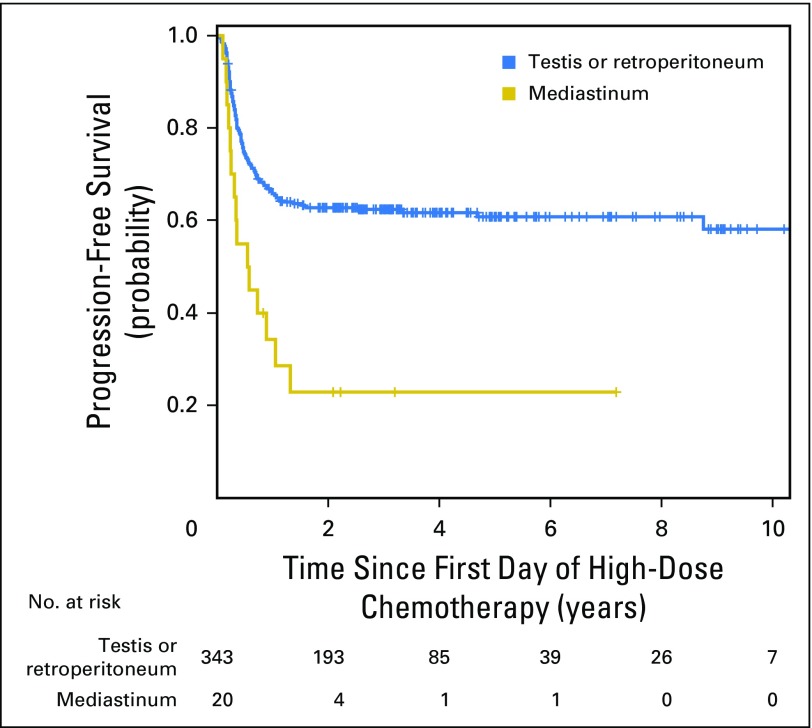
Purpose Patients with relapsed metastatic germ cell tumor (GCT) can be cured with second-line and even third-line regimens. We report survival outcomes of patients treated with high-dose chemotherapy (HDCT) and peripheral-blood stem-cell transplantation (PBSCT) at Indiana University between 2004 and 2014. Patients and Methods We conducted a retrospective analysis of 364 consecutive patients with GCT who progressed after cisplatin-based combination chemotherapy and were subsequently treated with HDCT and PBSCT. Three hundred forty-one patients received two consecutive courses of HDCT consisting of 700 mg/m2 carboplatin and 750 mg/m2 etoposide, each for 3 consecutive days, and each followed by PBSCT. Twenty-three patients received only a single course of HDCT because of progressive disease or toxicity. Cox proportional hazards models were used to test predictors of disease progression. Results The median age was 32 years (range, 17 to 70 years). With a median follow-up of 3.3 years, the 2-year progression-free survival (PFS) was 60% (95% CI, 55% to 65%) and the 2-year overall survival was 66% (95% CI, 60% to 70%). Three hundred three patients received HDCT as second-line therapy with a 2-year PFS of 63% (95% CI, 57% to 68%), and 61 patients received HDCT as third-line or later therapy with a 2-year PFS of 49% (95% CI, 36% to 61%). In a multivariable analysis, factors associated with disease progression included use of HDCT as third-line or later therapy, platinum-refractory disease, mediastinal primary tumor site, nonseminoma histology, intermediate- or poor-risk disease at the time of GCT diagnosis, and human chorionic gonadotropin ≥ 1,000 mIU/mL at initiation of HDCT. There were nine treatment-related deaths. Secondary leukemia developed in five patients. Conclusion This large single-institution study demonstrates that patients with relapsed metastatic GCT are curable by HDCT plus PBSCT even when used in third-line or later therapy.
Figures
Comment in
-
Testicular cancer: HDCT is an effective salvage approach.Nat Rev Urol. 2017 Feb;14(2):66. doi: 10.1038/nrurol.2016.256. Epub 2016 Dec 6. Nat Rev Urol. 2017. PMID: 27922039 No abstract available.
References
-
- Nigam M, Aschebrook-Kilfoy B, Shikanov S, et al. Increasing incidence of testicular cancer in the United States and Europe between 1992 and 2009. World J Urol. 2015;33:623–631. - PubMed
-
- Hanna NH, Einhorn LH. Testicular cancer—Discoveries and updates. N Engl J Med. 2014;371:2005–2016. - PubMed
-
- International Germ Cell Cancer Collaborative Group International Germ Cell Consensus Classification: A prognostic factor-based staging system for metastatic germ cell cancers. J Clin Oncol. 1997;15:594–603. - PubMed
-
- Adra N, Ku K, Kalra M, et al: Survival outcomes of patients with metastatic germ cell tumor (mGCT) treated from 1998 to 2012: The Indiana University (IU) experience. J Clin Oncol 34, 2016 (suppl 2S; abstr 491)
-
- Murphy BR, Breeden ES, Donohue JP, et al. Surgical salvage of chemorefractory germ cell tumors. J Clin Oncol. 1993;11:324–329. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
