

Impact of Extent of Resection on Local Control and Survival in Patients From the COG A3973 Study With High-Risk Neuroblastoma
- PMID: 27870572
- PMCID: PMC5455676
- DOI: 10.1200/JCO.2016.67.2642
Impact of Extent of Resection on Local Control and Survival in Patients From the COG A3973 Study With High-Risk Neuroblastoma
Abstract
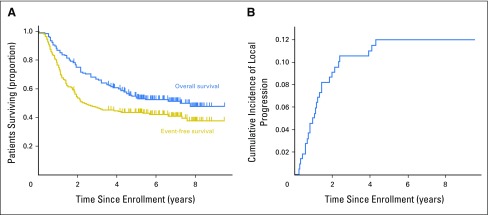
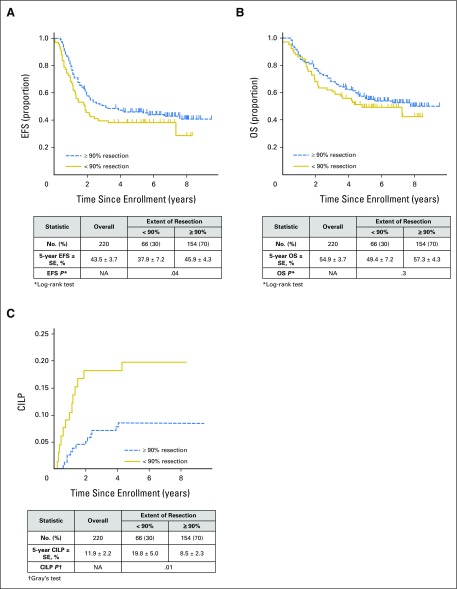
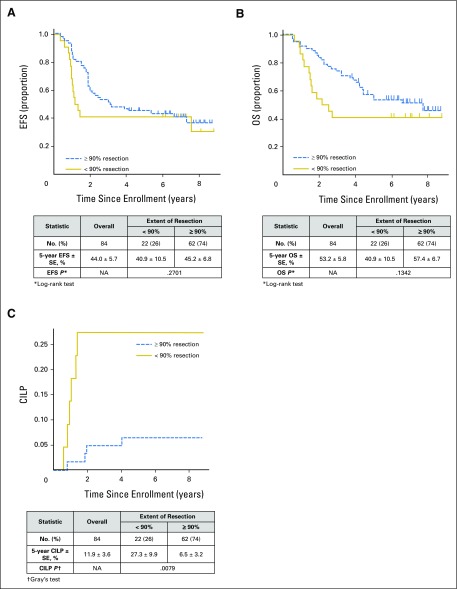
Purpose This analysis of patients in the Children's Oncology Group A3973 study evaluated the impact of extent of primary tumor resection on local progression and survival and assessed concordance between clinical and central imaging review-based assessments of resection extent. Patients and Methods The analytic cohort (n = 220) included patients who had both central surgery review and resection of the primary tumor site. For this analysis, resection categories of < 90% and ≥ 90% were used, with data on resection extent derived from operating surgeons' assessments (all patients), as well as blinded central imaging review of computed tomography scans for a subset of 84 patients; assessment results were compared for concordance. Treatment outcomes included event-free survival (EFS), overall survival (OS), and cumulative incidence of local progression (CILP). Results Surgeon-assessed extent of resection was ≥ 90% in 154 (70%) patients and < 90% in 66 (30%). Five-year EFS, OS, and CILP (± SE) were 43.5% ± 3.7%, 54.9% ± 3.7%, and 11.9% ± 2.2%, respectively. EFS was higher with ≥ 90% resection (45.9% ± 4.3%) than with < 90% resection (37.9% ± 7.2%; P = .04). Lower CILP ( P = .01) was associated with ≥ 90% resection (8.5% ± 2.3%) compared with < 90% resection (19.8% ± 5.0%). On multivariable analysis, ≥ 90% resection was associated with longer EFS after adjustment for MYCN amplification or diploidy but had no significant effect on OS. Concordance between surgeons' assessments of resection extent and central image-guided review was low, with agreement of 63% (< 90% v ≥ 90%; simple κ = -0.0301). Conclusion Despite discordance between clinical assessment of resection extent and assessment via central imaging review, a surgeon-assessed resection extent ≥ 90% was associated with significantly better EFS and lower CILP. Improving OS, however, remains a challenge in this disease. These findings support continued attempts at ≥ 90% resection of the primary tumor in high-risk neuroblastoma.
Figures
Comment in
-
Reply to J. Stenman et al.J Clin Oncol. 2017 Jun 10;35(17):1966-1967. doi: 10.1200/JCO.2017.72.2777. Epub 2017 Apr 19. J Clin Oncol. 2017. PMID: 28422554 No abstract available.
-
Improved Local Control by Extensive Surgery in High-Risk Neuroblastoma May Be Dependent on Adjuvant Radiotherapy.J Clin Oncol. 2017 Jun 10;35(17):1965-1966. doi: 10.1200/JCO.2016.72.1175. Epub 2017 Apr 19. J Clin Oncol. 2017. PMID: 28422555 No abstract available.
References
-
- Simon T, Häberle B, Hero B, et al. Role of surgery in the treatment of patients with stage 4 neuroblastoma age 18 months or older at diagnosis. J Clin Oncol. 2013;31:752–758. - PubMed
-
- Chamberlain RS, Quinones R, Dinndorf P, et al. Complete surgical resection combined with aggressive adjuvant chemotherapy and bone marrow transplantation prolongs survival in children with advanced neuroblastoma. Ann Surg Oncol. 1995;2:93–100. - PubMed
-
- Haase GM, O’Leary MC, Ramsay NK, et al: Aggressive surgery combined with intensive chemotherapy improves survival in poor-risk neuroblastoma. J Pediatr Surg 26:1119-1123, 1991; discussion 1123-1124 - PubMed
-
- Kaneko M, Ohakawa H, Iwakawa M. Is extensive surgery required for treatment of advanced neuroblastoma? J Pediatr Surg. 1997;32:1616–1619. - PubMed
-
- Kiely EM. Radical surgery for abdominal neuroblastoma. Semin Surg Oncol. 1993;9:489–492. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
