

Quantitative characterization of T-cell repertoire and biomarkers in kidney transplant rejection
- PMID: 27871261
- PMCID: PMC5117555
- DOI: 10.1186/s12882-016-0395-3
Quantitative characterization of T-cell repertoire and biomarkers in kidney transplant rejection
Abstract
Background: T-cell-mediated rejection (TCMR) remains a major cause of kidney allograft failure. The characterization of T-cell repertoire in different immunological disorders has emerged recently as a novel tool with significant implications. We herein sought to characterize T-cell repertoire using next generation sequencing to diagnose TCMR.
Methods: In this prospective study, we analyzed samples from 50 kidney transplant recipients. We collected blood and kidney transplant biopsy samples at sequential time points before and post transplant. We used next generation sequencing to characterize T-cell receptor (TCR) repertoire by using illumina miSeq on cDNA synthesized from RNA extracted from six patients' samples. We also measured RNA expression levels of FOXP3, CD8, CD4, granzyme and perforin in blood samples from all 50 patients.
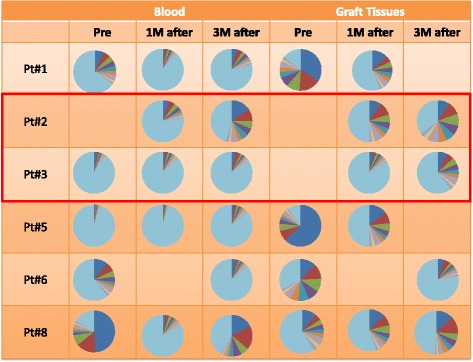
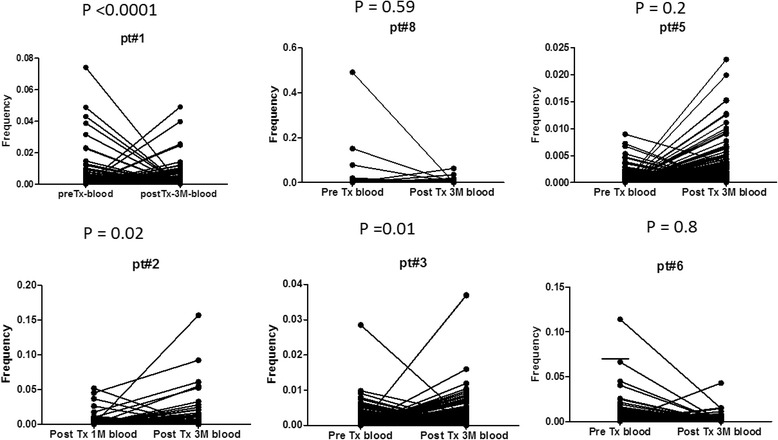
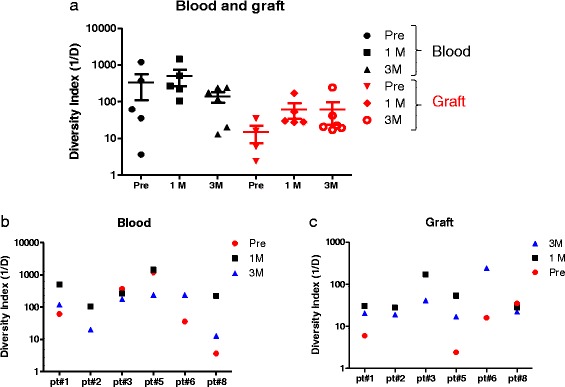
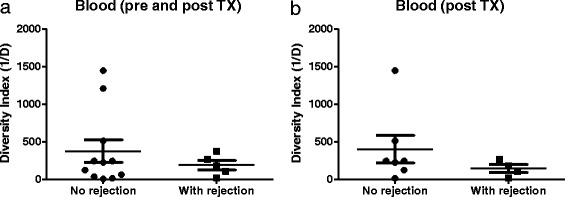
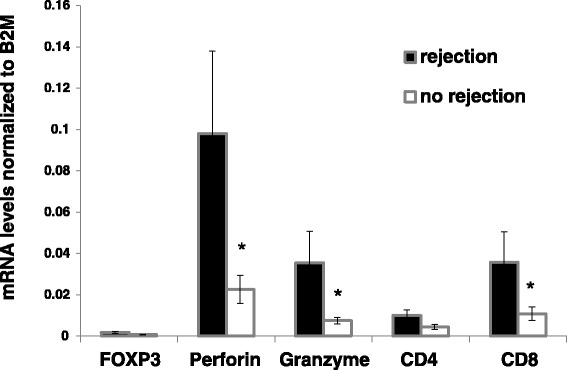
Results: Seven patients developed TCMR during the first three months of the study. Out of six patients who had complete sets of blood and biopsy samples two had TCMR. We found an expansion of the TCR repertoire in blood at time of rejection when compared to that at pre-transplant or one-month post transplant. Patients with TCMR (n = 7) had significantly higher RNA expression levels of FOXP3, Perforin, Granzyme, CD4 and CD8 in blood samples than those with no TCMR (n = 43) (P = 0.02, P = 0.003, P = 0.002, P = 0.017, and P = 0.01, respectively).
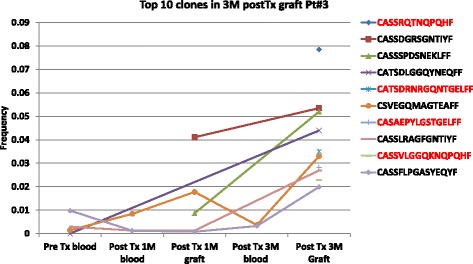
Conclusions: Our study provides a potential utilization of TCR clone kinetics analysis in the diagnosis of TCMR. This approach may allow for the identification of the expanded T-cell clones associated with the rejection and lead to potential noninvasive diagnosis and targeted therapies of TCMR.
Keywords: Kidney transplant; T cell mediated rejection; T cell sequencing; T-cell.
Figures
References
-
- Heng B, Li Y, Shi L, et al. A Meta-analysis of the Significance of Granzyme B and Perforin in Noninvasive Diagnosis of Acute Rejection After Kidney Transplantation. Transplantation. 2015;99:1477–86. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
