

Physical multimorbidity and psychosis: comprehensive cross sectional analysis including 242,952 people across 48 low- and middle-income countries
- PMID: 27871281
- PMCID: PMC5118890
- DOI: 10.1186/s12916-016-0734-z
Physical multimorbidity and psychosis: comprehensive cross sectional analysis including 242,952 people across 48 low- and middle-income countries
Abstract
Background: In people with psychosis, physical comorbidities, including cardiovascular and metabolic diseases, are highly prevalent and leading contributors to the premature mortality encountered. However, little is known about physical health multimorbidity in this population or in people with subclinical psychosis and in low- and middle-income countries (LMICs). This study explores physical health multimorbidity patterns among people with psychosis or subclinical psychosis.
Methods: Overall, data from 242,952 individuals from 48 LMICs, recruited via the World Health Survey, were included in this cross-sectional study. Participants were subdivided into those (1) with a lifetime diagnosis of psychosis ("psychosis"); (2) with more than one psychotic symptom in the past 12 months, but no lifetime diagnosis of psychosis ("subclinical psychosis"); and (3) without psychotic symptoms in the past 12 months or a lifetime diagnosis of psychosis ("controls"). Nine operationalized somatic disorders were examined: arthritis, angina pectoris, asthma, diabetes, chronic back pain, visual impairment, hearing problems, edentulism, and tuberculosis. The association between psychosis and multimorbidity was assessed by multivariable logistic regression analysis.
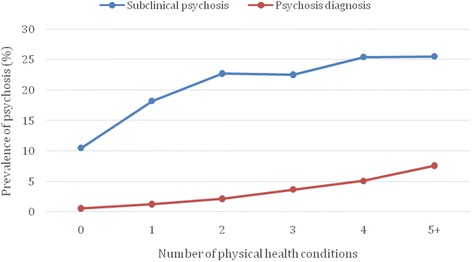
Results: The prevalence of multimorbidity (i.e., two or more physical health conditions) was: controls = 11.4% (95% CI, 11.0-11.8%); subclinical psychosis = 21.8% (95% CI, 20.6-23.0%), and psychosis = 36.0% (95% CI, 32.1-40.2%) (P < 0.0001). After adjustment for age, sex, education, country-wise wealth, and country, subclinical psychosis and psychosis were associated with 2.20 (95% CI, 2.02-2.39) and 4.05 (95% CI, 3.25-5.04) times higher odds for multimorbidity. Moreover, multimorbidity was increased in subclinical and established psychosis in all age ranges (18-44, 45-64, ≥ 65 years). However, multimorbidity was most evident in younger age groups, with people aged 18-44 years with psychosis at greatest odds of physical health multimorbidity (OR = 4.68; 95% CI, 3.46-6.32).
Conclusions: This large multinational study demonstrates that physical health multimorbidity is increased across the psychosis-spectrum. Most notably, the association between multimorbidity and psychosis was stronger among younger adults, thus adding further impetus to the calls for the early intervention efforts to prevent the burden of physical health comorbidity at later stages. Urgent public health interventions are necessary not only for those with a psychosis diagnosis, but also for subclinical psychosis to address this considerable public health problem.
Keywords: Metabolism; Multimorbidity; Physical health; Psychosis; Psychotic experiences.
Figures
Comment in
-
Multiple indicators of ill health are evident in people with psychosis.Evid Based Ment Health. 2018 Feb;21(1):e1-e2. doi: 10.1136/eb-2017-102647. Epub 2017 Oct 12. Evid Based Ment Health. 2018. PMID: 29025861 Free PMC article. No abstract available.
References
-
- Chang CK, Hayes RD, Broadbent M, Fernandes AC, Lee W, Hotopf M, et al. All-cause mortality among people with serious mental illness (SMI), substance use disorders, and depressive disorders in southeast London: a cohort study. BMC Psychiatry. 2010;10:77. doi: 10.1186/1471-244X-10-77. - DOI - PMC - PubMed
-
- Gardner-Sood P, Lally J, Smith S, Atakan Z, Ismail K, Greenwood KE, et al. Cardiovascular risk factors and metabolic syndrome in people with established psychotic illnesses: baseline data from the IMPaCT randomized controlled trial. Psychol Med. 2015;45(12):2619–29. doi: 10.1017/S0033291715000562. - DOI - PMC - PubMed
-
- Vancampfort D, Stubbs B, Mitchell AJ, De Hert M, Wampers M, Ward PB, et al. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: a systematic review and meta-analysis. World Psychiatry. 2015;14(3):339–47. doi: 10.1002/wps.20252. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
