

Tumor control probability modeling for stereotactic body radiation therapy of early-stage lung cancer using multiple bio-physical models
- PMID: 27871671
- PMCID: PMC5649355
- DOI: 10.1016/j.radonc.2016.11.006
Tumor control probability modeling for stereotactic body radiation therapy of early-stage lung cancer using multiple bio-physical models
Abstract
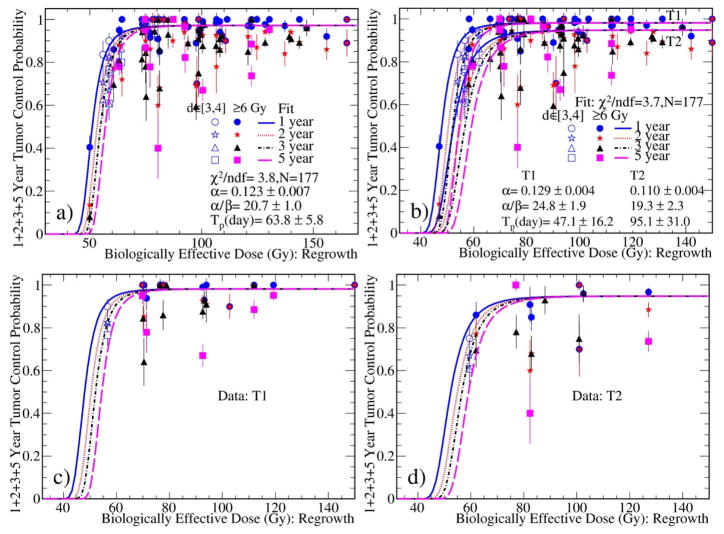
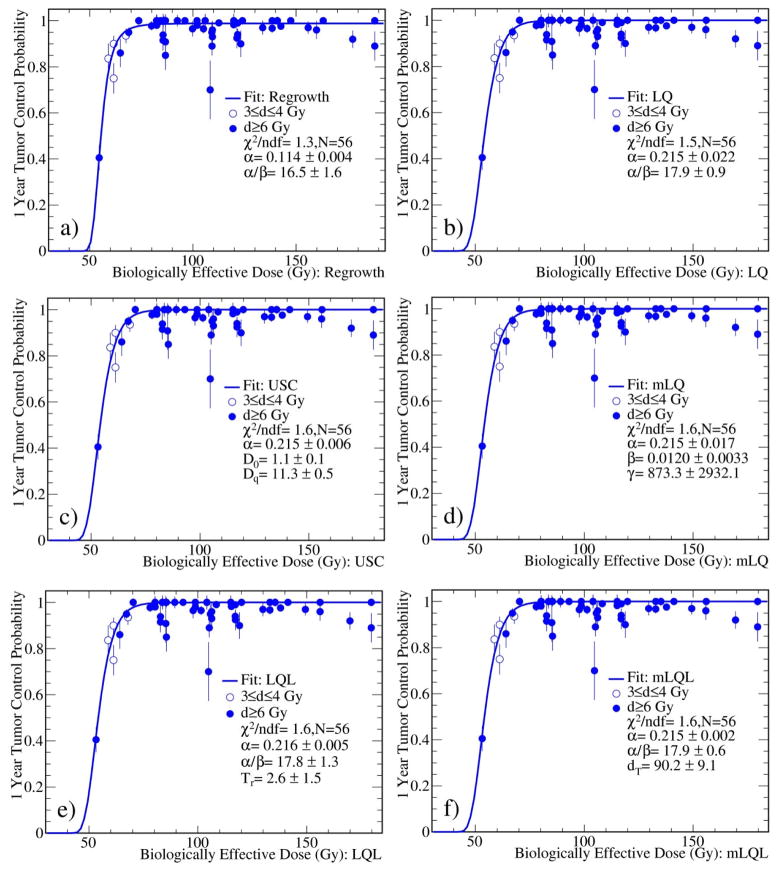
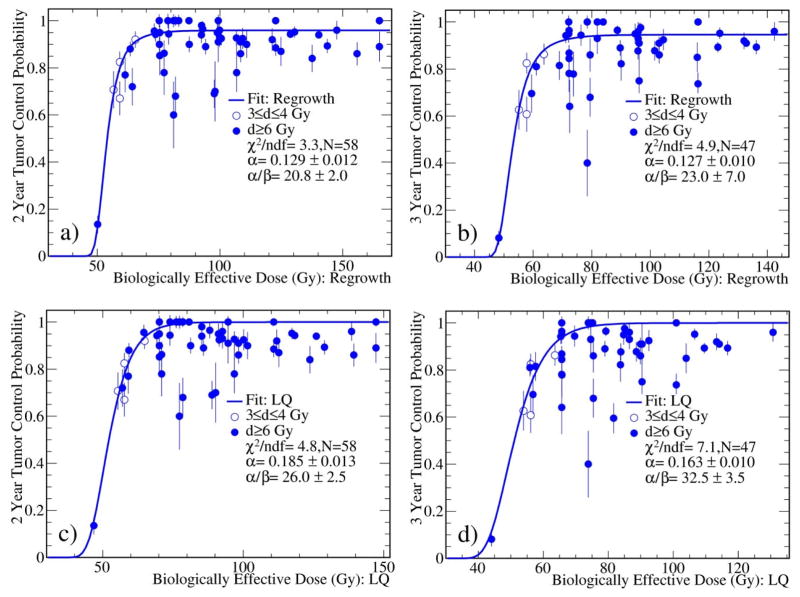
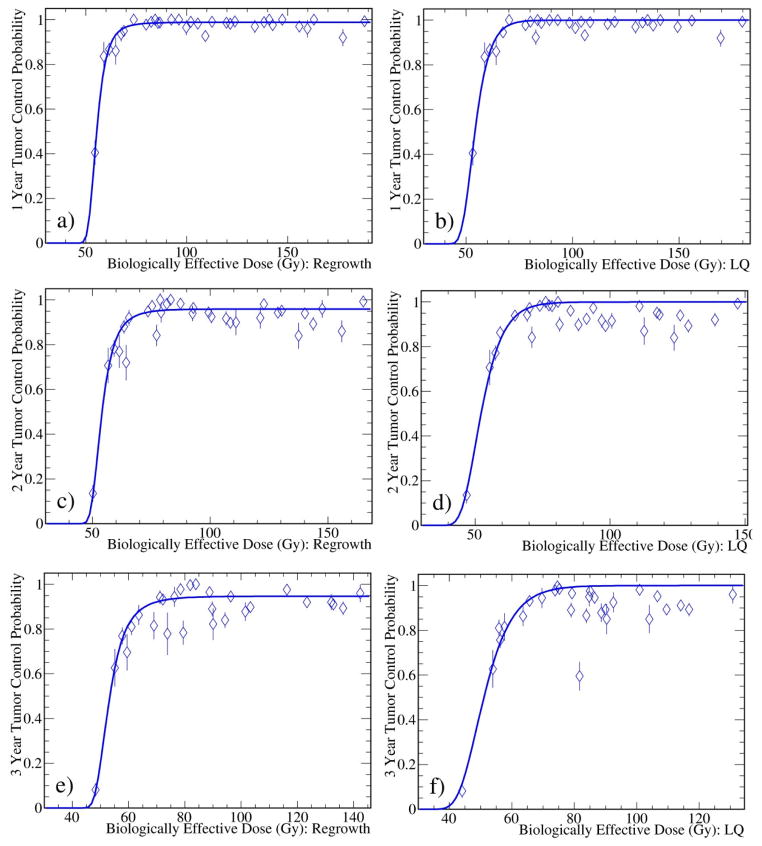
This work is to analyze pooled clinical data using different radiobiological models and to understand the relationship between biologically effective dose (BED) and tumor control probability (TCP) for stereotactic body radiotherapy (SBRT) of early-stage non-small cell lung cancer (NSCLC). The clinical data of 1-, 2-, 3-, and 5-year actuarial or Kaplan-Meier TCP from 46 selected studies were collected for SBRT of NSCLC in the literature. The TCP data were separated for Stage T1 and T2 tumors if possible, otherwise collected for combined stages. BED was calculated at isocenters using six radiobiological models. For each model, the independent model parameters were determined from a fit to the TCP data using the least chi-square (χ2) method with either one set of parameters regardless of tumor stages or two sets for T1 and T2 tumors separately. The fits to the clinic data yield consistent results of large α/β ratios of about 20Gy for all models investigated. The regrowth model that accounts for the tumor repopulation and heterogeneity leads to a better fit to the data, compared to other 5 models where the fits were indistinguishable between the models. The models based on the fitting parameters predict that the T2 tumors require about additional 1Gy physical dose at isocenters per fraction (⩽5 fractions) to achieve the optimal TCP when compared to the T1 tumors. In conclusion, this systematic analysis of a large set of published clinical data using different radiobiological models shows that local TCP for SBRT of early-stage NSCLC has strong dependence on BED with large α/β ratios of about 20Gy. The six models predict that a BED (calculated with α/β of 20) of 90Gy is sufficient to achieve TCP⩾95%. Among the models considered, the regrowth model leads to a better fit to the clinical data.
Keywords: Early stage non-small cell lung cancer; Stereotactic body radiation therapy; Tumor control probability modeling.
Copyright © 2016 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
There is no conflict of interest for all authors.
Figures
References
-
- Mountain CF. Surgical treatment of lung cancer. Crit Rev Oncol hematol. 1991;11:179–207. - PubMed
-
- Dominioni L, Imperatori A, Rovera F, et al. Stage I nonsmall cell lung carcinoma: Analysis of survival and implications for screening. Cancer. 2000;89:S2334–S2344. - PubMed
-
- Qiao X, Tullgren O, Lax I, et al. The role of radiotherapy in treatment of stage I non-small cell lung cancer. Lung cancer. 2003;41:1–11. - PubMed
-
- Robinson CG, DeWees TA, El Naqa IM, et al. Patterns of failure after stereotactic body radiation therapy or lobar resection for clinical stage I non-small-cell lung cancer. J Thorac Oncol. 2013;8:192–201. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
