

Lung neuroendocrine tumours: deep sequencing of the four World Health Organization histotypes reveals chromatin-remodelling genes as major players and a prognostic role for TERT, RB1, MEN1 and KMT2D
- PMID: 27873319
- PMCID: PMC5324596
- DOI: 10.1002/path.4853
Lung neuroendocrine tumours: deep sequencing of the four World Health Organization histotypes reveals chromatin-remodelling genes as major players and a prognostic role for TERT, RB1, MEN1 and KMT2D
Abstract
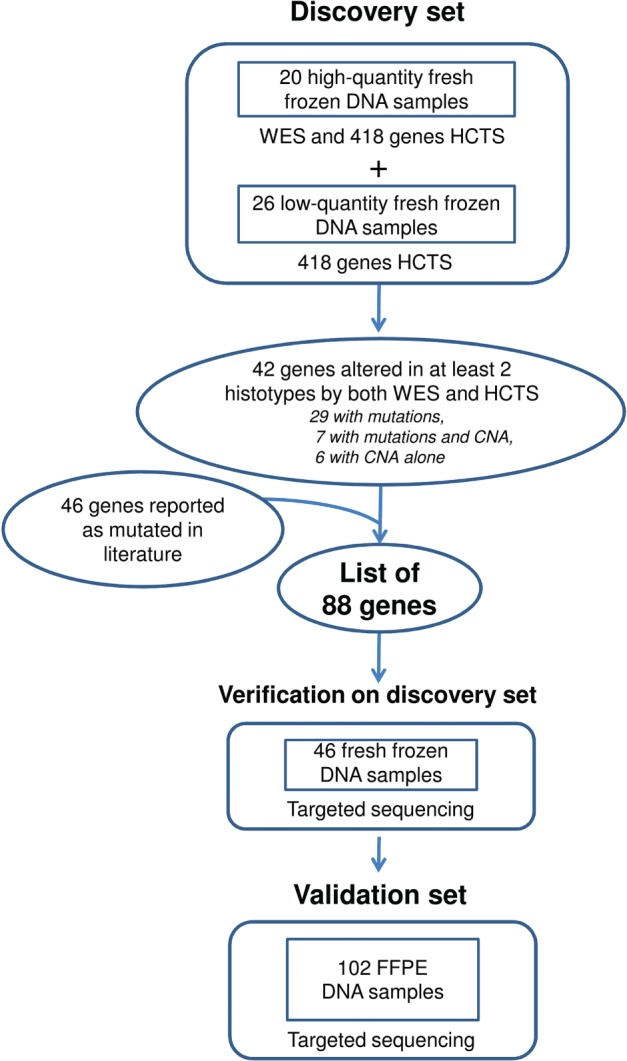
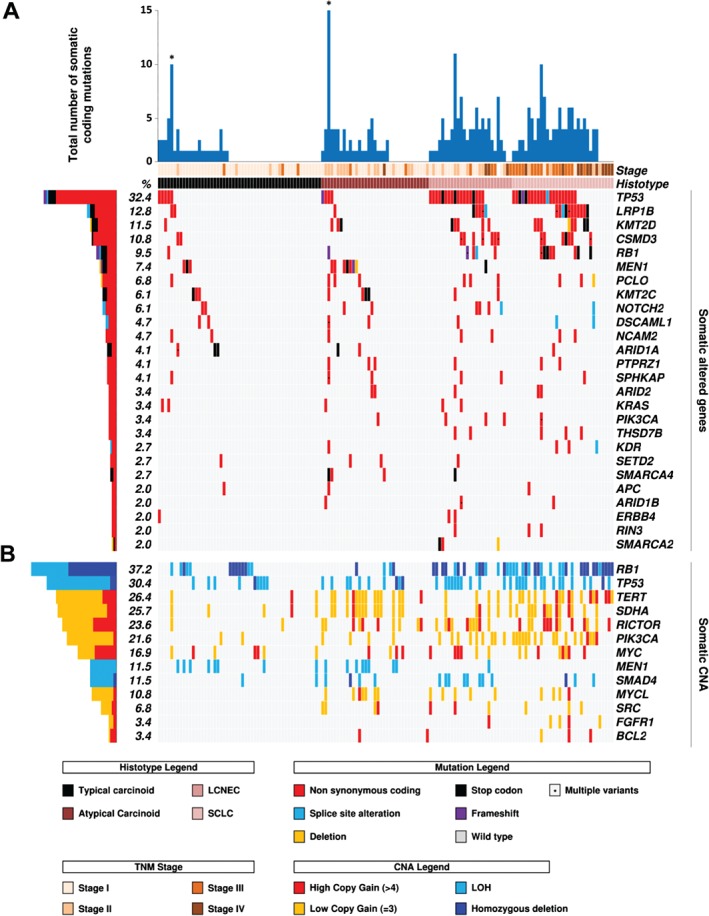
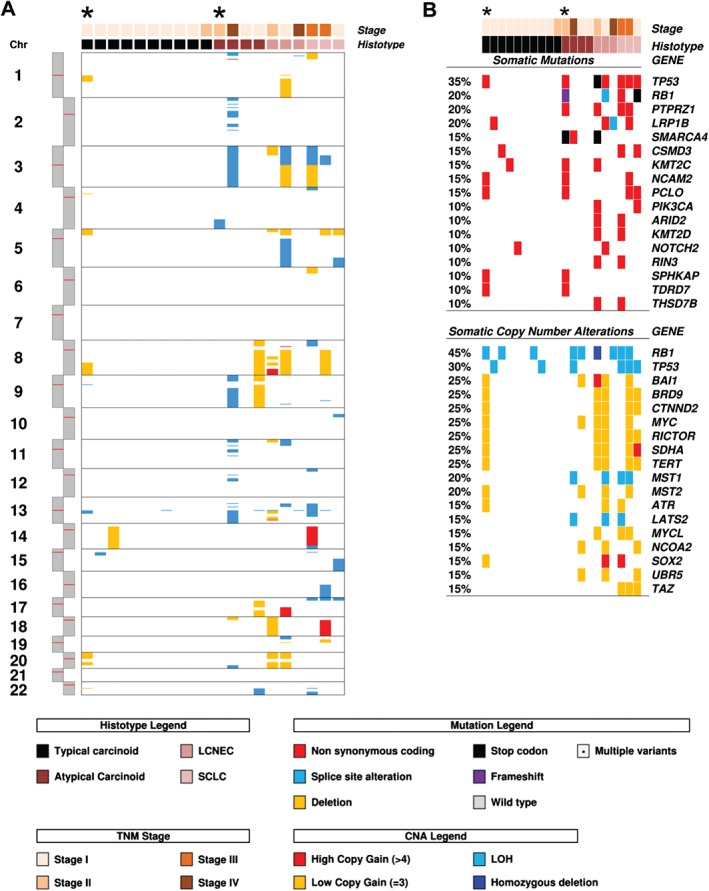
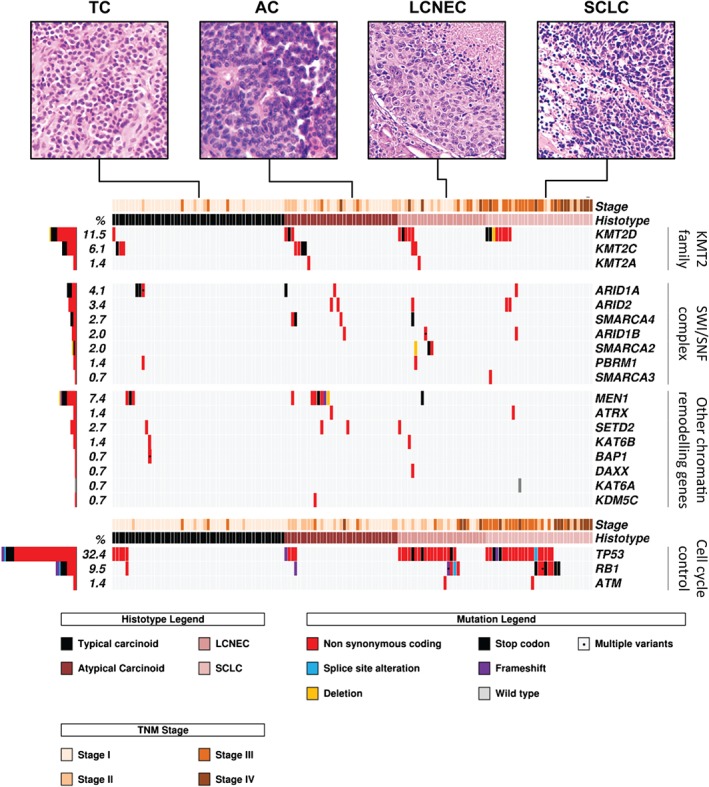
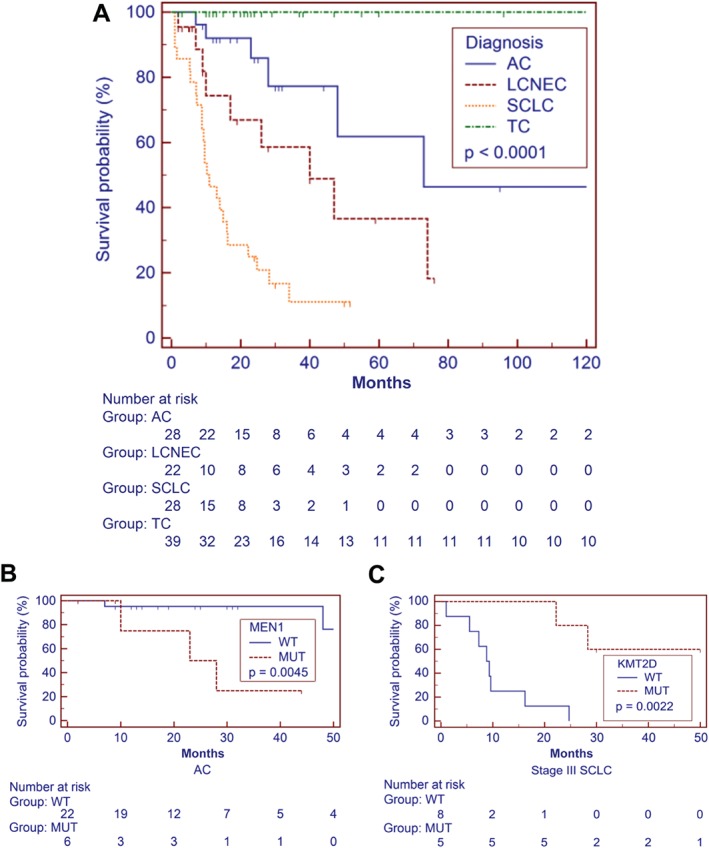
Next-generation sequencing (NGS) was applied to 148 lung neuroendocrine tumours (LNETs) comprising the four World Health Organization classification categories: 53 typical carcinoid (TCs), 35 atypical carcinoid (ACs), 27 large-cell neuroendocrine carcinomas, and 33 small-cell lung carcinomas. A discovery screen was conducted on 46 samples by the use of whole-exome sequencing and high-coverage targeted sequencing of 418 genes. Eighty-eight recurrently mutated genes from both the discovery screen and current literature were verified in the 46 cases of the discovery screen, and validated on additional 102 LNETs by targeted NGS; their prevalence was then evaluated on the whole series. Thirteen of these 88 genes were also evaluated for copy number alterations (CNAs). Carcinoids and carcinomas shared most of the altered genes but with different prevalence rates. When mutations and copy number changes were combined, MEN1 alterations were almost exclusive to carcinoids, whereas alterations of TP53 and RB1 cell cycle regulation genes and PI3K/AKT/mTOR pathway genes were significantly enriched in carcinomas. Conversely, mutations in chromatin-remodelling genes, including those encoding histone modifiers and members of SWI-SNF complexes, were found at similar rates in carcinoids (45.5%) and carcinomas (55.0%), suggesting a major role in LNET pathogenesis. One AC and one TC showed a hypermutated profile associated with a POLQ damaging mutation. There were fewer CNAs in carcinoids than in carcinomas; however ACs showed a hybrid pattern, whereby gains of TERT, SDHA, RICTOR, PIK3CA, MYCL and SRC were found at rates similar to those in carcinomas, whereas the MEN1 loss rate mirrored that of TCs. Multivariate survival analysis revealed RB1 mutation (p = 0.0005) and TERT copy gain (p = 0.016) as independent predictors of poorer prognosis. MEN1 mutation was associated with poor prognosis in AC (p = 0.0045), whereas KMT2D mutation correlated with longer survival in SCLC (p = 0.0022). In conclusion, molecular profiling may complement histology for better diagnostic definition and prognostic stratification of LNETs. © 2016 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Keywords: KMT2D; MEN1; RB1; TERT; exome sequencing; lung tumours; neuroendocrine; targeted sequencing.
© 2016 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Figures
References
-
- Travis WD, Brambilla E, Burke AP, et al (eds). World Health Organization Classification of Tumours of the Lung, Pleura, Thymus and Heart, 4th edn. IARC Press: Lyon, 2015. - PubMed
-
- Travis WD, Rush W, Flieder DB, et al Survival analysis of 200 pulmonary neuroendocrine tumors with clarification of criteria for atypical carcinoid and its separation from typical carcinoid. Am J Surg Pathol 1998; 22 : 934–944. - PubMed
-
- Asamura H, Kameya T, Matsuno Y, et al Neuroendocrine neoplasms of the lung: a prognostic spectrum. J Clin Oncol 2006; 24 : 70–76. - PubMed
-
- Righi L, Volante M, Tavaglione V, et al Somatostatin receptor tissue distribution in lung neuroendocrine tumours: a clinicopathologic and immunohistochemical study of 218 ‘clinically aggressive’ cases. Ann Oncol 2010; 21 : 548–555. - PubMed
-
- Rindi G, Klersy C, Inzani F, et al Grading the neuroendocrine tumors of the lung: an evidence‐based proposal. Endocr Relat Cancer 2014; 21 : 1–16. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
