

Cyclosporine Sparing Effect of Enteric-Coated Mycophenolate Sodium in De Novo Kidney Transplantation
- PMID: 27873516
- PMCID: PMC5122640
- DOI: 10.3349/ymj.2017.58.1.217
Cyclosporine Sparing Effect of Enteric-Coated Mycophenolate Sodium in De Novo Kidney Transplantation
Abstract
Purpose: The increased tolerability of enteric-coated mycophenolate sodium (EC-MPS), compared to mycophenolate mofetil, among kidney transplant recipients has the potential to facilitate cyclosporine (CsA) minimization. Therefore, a prospective trial to determine the optimum EC-MPS dose in CsA-based immunosuppression regimens is necessary.
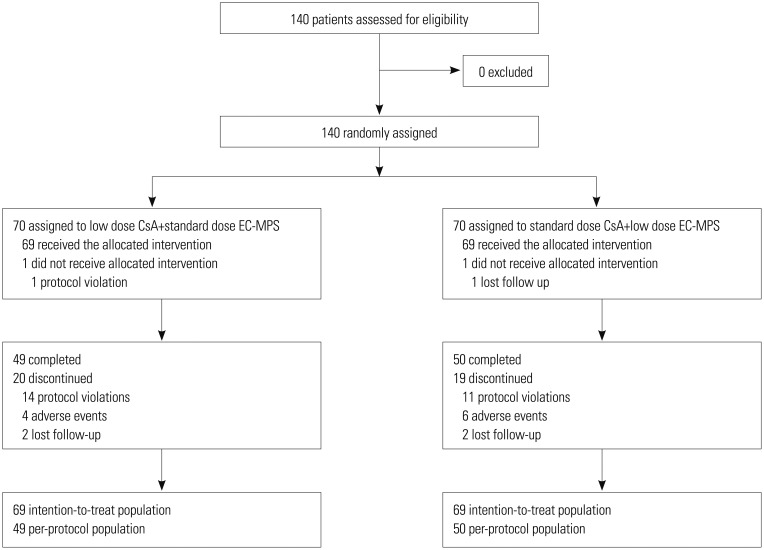
Materials and methods: A comparative, parallel, randomized, open-label study was performed for 140 patients from four centers to compare the efficacy and tolerability of low dose CsA with standard dose EC-MPS (the investigational group) versus standard dose CsA with low dose EC-MPS (the control group) for six months in de novo kidney transplant recipients. Graft function, the incidence of efficacy failure [biopsy-confirmed acute rejection (BCAR), death, graft loss, loss to follow-up], and adverse events were compared.
Results: The mean estimated glomerular filtration rate (eGFR) of the investigational group at six months post-transplantation was non-inferior to that of the control group (confidence interval between 57.3 mL/min/1.73m² and 67.4 mL/min/1.73 m², p<0.001). One graft loss was reported in the control group, and no patient deaths were reported in either group. The incidence of BCAR of the investigational group was 8.7%, compared to 18.8% in the control group (p=0.137), during the study period. There were no significant differences (p>0.05) in the incidence of discontinuations and serious adverse events (SAE) between the groups.
Conclusion: CsA minimization using a standard dose of EC-MPS kept the incidence of acute rejection and additional risks as low as conventional immunosuppression and provided therapeutic equivalence in terms of renal graft function and safety issues.
Keywords: Enteric-coated mycophenolate sodium; cyclosporine; immunosuppression.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures

References
-
- Tantravahi J, Womer KL, Kaplan B. Why hasn't eliminating acute rejection improved graft survival? Annu Rev Med. 2007;58:369–385. - PubMed
-
- Meier-Kriesche HU, Schold JD, Srinivas TR, Kaplan B. Lack of improvement in renal allograft survival despite a marked decrease in acute rejection rates over the most recent era. Am J Transplant. 2004;4:378–383. - PubMed
-
- Meier-Kriesche HU, Schold JD, Kaplan B. Long-term renal allograft survival: have we made significant progress or is it time to rethink our analytic and therapeutic strategies? Am J Transplant. 2004;4:1289–1295. - PubMed
-
- Nankivell BJ, Borrows RJ, Fung CL, O'Connell PJ, Chapman JR, Allen RD. Calcineurin inhibitor nephrotoxicity: longitudinal assessment by protocol histology. Transplantation. 2004;78:557–565. - PubMed
-
- Bolin P, Tanriover B, Zibari GB, Lynn ML, Pirsch JD, Chan L, et al. Improvement in 3-month patient-reported gastrointestinal symptoms after conversion from mycophenolate mofetil to entericcoated mycophenolate sodium in renal transplant patients. Transplantation. 2007;84:1443–1451. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
