

Relationship Between Age and Trajectories of Rehospitalization Risk in Older Adults
- PMID: 27874977
- PMCID: PMC5310961
- DOI: 10.1111/jgs.14583
Relationship Between Age and Trajectories of Rehospitalization Risk in Older Adults
Abstract
Objectives: To characterize the magnitude and duration of risk of rehospitalization according to age after hospitalization for heart failure (HF), acute myocardial infarction (AMI), or pneumonia.
Design: Retrospective cohort study.
Setting: U.S. hospitals (n = 4,767).
Participants: All Medicare fee-for-service beneficiaries aged 65 and older surviving hospitalization for HF, AMI, or pneumonia between October 2012 and December 2013.
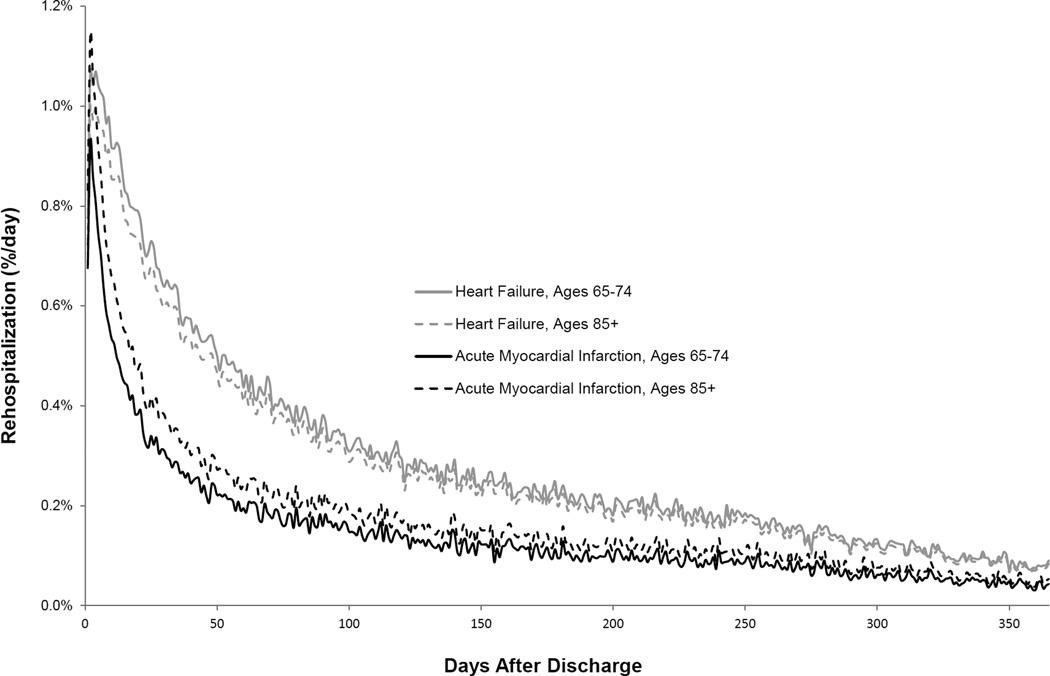
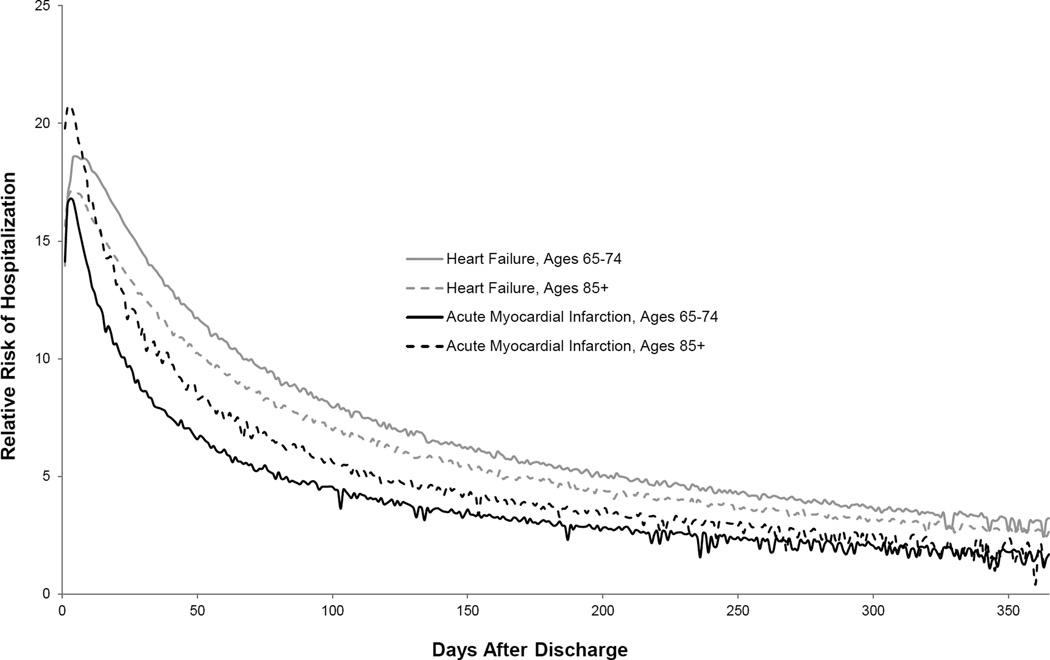
Measurements: Daily risk of first rehospitalization for 1 year after hospital discharge was calculated according to age category (65-74, 75-84, ≥85) after adjustment for sex, race, comorbidities, and median ZIP code income. Time required for adjusted rehospitalization risk to decline 50% from maximum value after discharge, time required for adjusted risk to approach a plateau period of minimal day-to-day change, and degree to which adjusted risk was higher in recently hospitalized individuals than in the general elderly population were identified.
Results: There were 414,720 hospitalizations for HF, 177,752 for AMI, and 568,304 for pneumonia. The adjusted risk of rehospitalization declined with increasing age after HF hospitalization (P < .001), rose with increasing age after AMI hospitalization (P < .001), and was slightly lower with increasing age after pneumonia hospitalization (P = .002). Adjusted risks of rehospitalization were high beyond 30 days after hospitalization for all ages.
Conclusion: Although older age has heterogeneous relationships with rehospitalization risk, risk of readmission remains high for an extended time after discharge regardless of age or admitting condition. Condition-specific data on risk can be used to guide discussions on advanced care planning and strategies for longitudinal follow-up after hospitalization.
Keywords: cardiovascular disease; geriatrics; pulmonary diseases; quality of care; readmission.
© 2016, Copyright the Authors Journal compilation © 2016, The American Geriatrics Society.
Conflict of interest statement
Kumar Dharmarajan : Employment or affiliation:works under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures ; Grants/funds: no; Honoraria: no; Speaker forum: no; Consultant:consultant for Clover Health ; Stocks: no; Royalties: no; Expert testimony: no; Board member:member of a scientific advisory board for Clover Health ; Patents: no; Personal relationship: noAngela Hsieh : Employment or affiliation: no; Grants/funds: no; Honoraria: no; Speaker forum: no; Consultant: no; Stocks: no; Royalties: no; Expert testimony: no; Board member: no; Patents: no; Personal relationship: noRachel P. Dreyer : Employment or affiliation: no; Grants/funds: no; Honoraria: no; Speaker forum: no; Consultant: no; Stocks: no; Royalties: no; Expert testimony: no; Board member: no; Patents: no; Personal relationship: noJack Welsh : Employment or affiliation: no; Grants/funds: no; Honoraria: no; Speaker forum: no; Consultant: no; Stocks: no; Royalties: no; Expert testimony: no; Board member: no; Patents: no; Personal relationship: noLi Qin : Employment or affiliation:works under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures ; Grants/funds: no; Honoraria: no; Speaker forum: no; Consultant: no; Stocks: no; Royalties: no; Expert testimony: no; Board member: no; Patents: no; Personal relationship: noHarlan M. Krumholz : Employment or affiliation:works under contract with the Centers for Medicare & Medicaid Services to develop and maintain performance measures ; Grants/funds:recipient of research grants from Medtronic and Johnson & Johnson, through Yale University, to develop methods of clinical trial data sharing ; Honoraria: no; Speaker forum: no; Consultant: no; Stocks: no; Royalties: no; Expert testimony: no; Board member:chair of a cardiac scientific advisory board for UnitedHealth ; Patents: no; Personal relationship: no
Figures
Similar articles
-
Trajectories of risk after hospitalization for heart failure, acute myocardial infarction, or pneumonia: retrospective cohort study.BMJ. 2015 Feb 5;350:h411. doi: 10.1136/bmj.h411. BMJ. 2015. PMID: 25656852 Free PMC article.
-
Sex Differences in Trajectories of Risk After Rehospitalization for Heart Failure, Acute Myocardial Infarction, or Pneumonia.Circ Cardiovasc Qual Outcomes. 2017 May;10(5):e003271. doi: 10.1161/CIRCOUTCOMES.116.003271. Circ Cardiovasc Qual Outcomes. 2017. PMID: 28506980 Free PMC article.
-
Trajectories of Risk for Specific Readmission Diagnoses after Hospitalization for Heart Failure, Acute Myocardial Infarction, or Pneumonia.PLoS One. 2016 Oct 7;11(10):e0160492. doi: 10.1371/journal.pone.0160492. eCollection 2016. PLoS One. 2016. PMID: 27716841 Free PMC article.
-
Cognitive impairment and 30-day rehospitalization rate in patients with acute heart failure: A systematic review and meta-analysis.Indian Heart J. 2019 Jan-Feb;71(1):52-59. doi: 10.1016/j.ihj.2018.12.006. Epub 2019 Jan 3. Indian Heart J. 2019. PMID: 31000183 Free PMC article.
-
Association Between Cirrhosis and 30-Day Rehospitalization After Index Hospitalization for Heart Failure.Curr Probl Cardiol. 2022 Oct;47(10):100993. doi: 10.1016/j.cpcardiol.2021.100993. Epub 2021 Sep 24. Curr Probl Cardiol. 2022. PMID: 34571101 Review.
Cited by
-
180-day readmission risk model for older adults with acute myocardial infarction: the SILVER-AMI study.Open Heart. 2021 Jan;8(1):e001442. doi: 10.1136/openhrt-2020-001442. Open Heart. 2021. PMID: 33452007 Free PMC article.
-
Readmissions of adults within three age groups following hospitalization for pneumonia: Analysis from the Nationwide Readmissions Database.PLoS One. 2018 Sep 13;13(9):e0203375. doi: 10.1371/journal.pone.0203375. eCollection 2018. PLoS One. 2018. PMID: 30212485 Free PMC article. Clinical Trial.
-
Risk-adjusted outcomes of inpatient medicare medical admissions.Medicine (Baltimore). 2018 Sep;97(37):e12269. doi: 10.1097/MD.0000000000012269. Medicine (Baltimore). 2018. PMID: 30212962 Free PMC article.
-
Epidemiology, pathophysiology, and prognosis of heart failure in the elderly.Heart Fail Clin. 2007 Oct;3(4):381-7. doi: 10.1016/j.hfc.2007.07.004. Heart Fail Clin. 2007. PMID: 17905375 Free PMC article.
-
Readmissions Following a Hospitalization for Cardiovascular Events in Dialysis Patients: A Retrospective Cohort Study.J Am Heart Assoc. 2018 Feb 13;7(4):e007231. doi: 10.1161/JAHA.117.007231. J Am Heart Assoc. 2018. PMID: 29440035 Free PMC article.
References
-
- Ross JS, Mulvey GK, Stauffer B, et al. Statistical models and patient predictors of readmission for heart failure: a systematic review. Arch Intern Med. 2008;168:1371–1386. - PubMed
-
- Desai MM, Stauffer BD, Feringa HH, et al. Statistical models and patient predictors of readmission for acute myocardial infarction: a systematic review. Circ Cardiovasc Qual Outcomes. 2009;2:500–507. - PubMed
-
- Kocher RP, Adashi EY. Hospital readmissions and the Affordable Care Act: paying for coordinated quality care. JAMA. 2011;306:1794–1795. - PubMed
-
- Keenan PS, Normand SL, Lin Z, et al. An administrative claims measure suitable for profiling hospital performance on the basis of 30-day all-cause readmission rates among patients with heart failure. Circ Cardiovasc Qual Outcomes. 2008;1:29–37. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
