

Socioeconomic Status and Poor Health Outcome at 10 Years of Follow-Up in the Multi-Ethnic Study of Atherosclerosis
- PMID: 27875557
- PMCID: PMC5119729
- DOI: 10.1371/journal.pone.0165651
Socioeconomic Status and Poor Health Outcome at 10 Years of Follow-Up in the Multi-Ethnic Study of Atherosclerosis
Abstract
Background/objectives: Predictors of healthy aging have not been well-studied using longitudinal data with demographic, clinical, subclinical, and genetic information. The objective was to identify predictors of poor health outcome at 10 years of follow-up in the Multi-Ethnic Study of Atherosclerosis (MESA).
Design: Prospective cohort study.
Setting: Population-based sample from 6 U.S. communities.
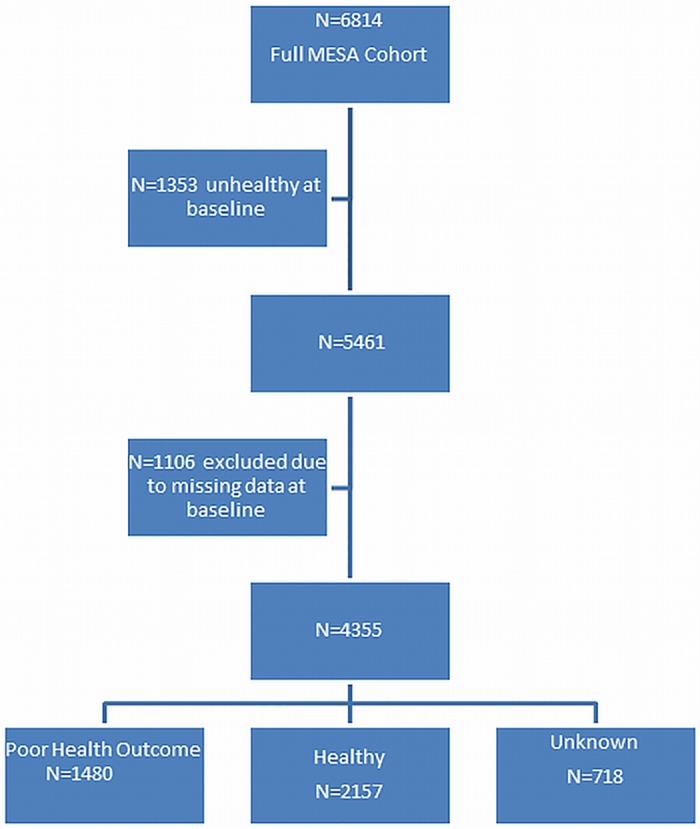
Participants: 4,355 participants In the MESA Study.
Measurements: Poor health outcome at 10 years of follow-up was defined as having died or having clinical cardiovascular disease, depression, cognitive impairment, chronic obstructive pulmonary disease, or cancer other than non-melanoma skin cancer. Absolute risk regression was used to estimate risk differences in the outcome adjusting for demographic variables, clinical and behavioral risk factors, subclinical cardiovascular disease, and ApoE genotype. Models were weighted to account for selective attrition.
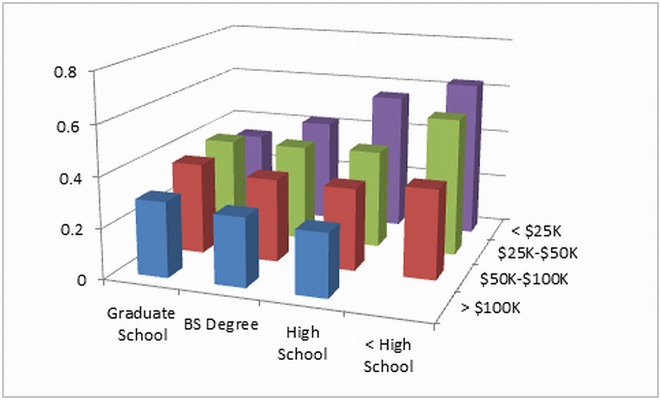
Results: Mean age at 10 years of follow-up was 69.5 years; 1,480 participants had a poor health outcome, 2,157 participants were in good health, and 718 were unknown. Older age, smoking, not taking a statin, hypertension, diabetes, and higher coronary calcium score were associated with higher probability of poor health outcome. After multivariable adjustment, participants in the lowest income and educational categories had 7 to 14% greater absolute risk of poor health outcome at 10 years of follow-up compared to those in the next highest categories of income or education (P = 0.002 for both). Those in the lowest categories of both income and education had 21% greater absolute risk of poor health outcome compared to those in the highest categories of both income and education.
Conclusions: Low income and educational level predict poor health outcome at 10 years of follow-up in an aging cohort, independent of clinical and behavioral risk factors and subclinical cardiovascular disease.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Association Between Self-rated Health, Coronary Artery Calcium Scores, and Atherosclerotic Cardiovascular Disease Risk: The Multi-Ethnic Study of Atherosclerosis (MESA).JAMA Netw Open. 2019 Feb 1;2(2):e188023. doi: 10.1001/jamanetworkopen.2018.8023. JAMA Netw Open. 2019. PMID: 30768193 Free PMC article.
-
Sociodemographic Correlates of Cognition in the Multi-Ethnic Study of Atherosclerosis (MESA).Am J Geriatr Psychiatry. 2015 Jul;23(7):684-97. doi: 10.1016/j.jagp.2015.01.003. Epub 2015 Jan 20. Am J Geriatr Psychiatry. 2015. PMID: 25704999 Free PMC article.
-
Ten-year association of coronary artery calcium with atherosclerotic cardiovascular disease (ASCVD) events: the multi-ethnic study of atherosclerosis (MESA).Eur Heart J. 2018 Jul 1;39(25):2401-2408. doi: 10.1093/eurheartj/ehy217. Eur Heart J. 2018. PMID: 29688297 Free PMC article.
-
Behavioral and Pharmacotherapy Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults: An Updated Systematic Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. PMID: 30354042 Free Books & Documents. Review.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Socioeconomic inequality in unmet outpatient healthcare needs among people living in urban informal settlements in Sanandaj city, Iran.Int J Equity Health. 2023 Dec 11;22(1):257. doi: 10.1186/s12939-023-02076-1. Int J Equity Health. 2023. PMID: 38082298 Free PMC article.
-
Effects of socioeconomic factors on cardiovascular-related symptoms among residents in Fukushima after the Great East Japan Earthquake: a cross-sectional study using data from the Fukushima Health Management Survey.BMJ Open. 2017 Jun 23;7(6):e014077. doi: 10.1136/bmjopen-2016-014077. BMJ Open. 2017. PMID: 28645951 Free PMC article.
-
Barriers to blood pressure control initiatives: Regional diversity, inadequate measurement techniques, guideline inconsistencies, and health disparities.J Clin Hypertens (Greenwich). 2019 Feb;21(2):204-207. doi: 10.1111/jch.13466. Epub 2019 Jan 4. J Clin Hypertens (Greenwich). 2019. PMID: 30609230 Free PMC article. No abstract available.
-
Outpatient primary and tertiary healthcare utilisation among public rental housing residents in Singapore.BMC Health Serv Res. 2019 Apr 15;19(1):227. doi: 10.1186/s12913-019-4047-8. BMC Health Serv Res. 2019. PMID: 30987617 Free PMC article.
-
Prevalence and Distribution of Atherosclerosis in a Low- to Intermediate-Risk Population: Assessment with Whole-Body MR Angiography.Radiology. 2018 Jun;287(3):795-804. doi: 10.1148/radiol.2018171609. Epub 2018 May 1. Radiology. 2018. PMID: 29714681 Free PMC article.
References
-
- He W, Muenchrath MN. 90+ in the United States: 2006–2008. US Census Bureau, 2011.
-
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol Series A, Biological Sciences and Medical Sciences. 2001;56: M146–M157. - PubMed
Publication types
MeSH terms
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095168/HL/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095166/HL/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- R01 HL076831/HL/NHLBI NIH HHS/United States
- N01 HC095167/HL/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
