

Sleep-related hypermotor epilepsy: Long-term outcome in a large cohort
- PMID: 27881627
- PMCID: PMC5200852
- DOI: 10.1212/WNL.0000000000003459
Sleep-related hypermotor epilepsy: Long-term outcome in a large cohort
Abstract
Objective: To assess the long-term outcome of sleep-related hypermotor epilepsy (SHE).
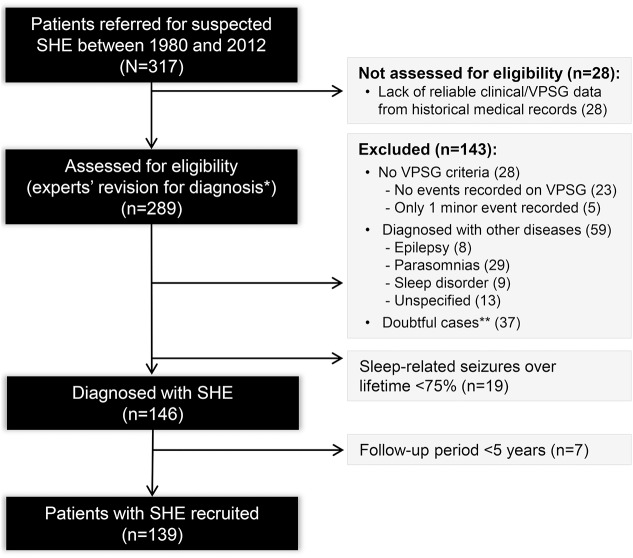
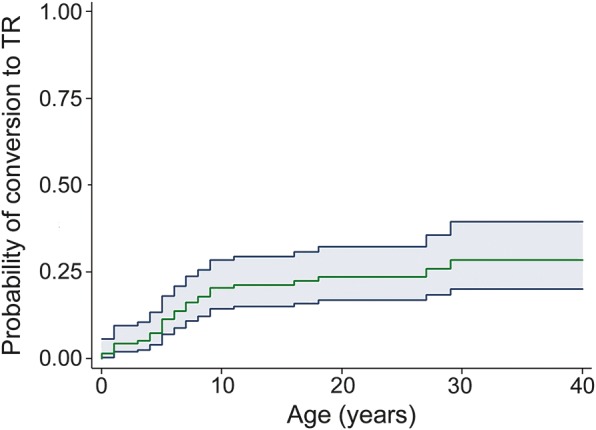
Methods: We retrospectively reconstructed a representative cohort of patients diagnosed with SHE according to international diagnostic criteria, sleep-related seizures ≥75% and follow-up ≥5 years. Terminal remission (TR) was defined as a period of ≥5 consecutive years of seizure freedom at the last follow-up. We used Kaplan-Meier estimates to calculate the cumulative time-dependent probability of TR and to generate survival curves. Univariate and multivariate Cox regression analyses were performed.
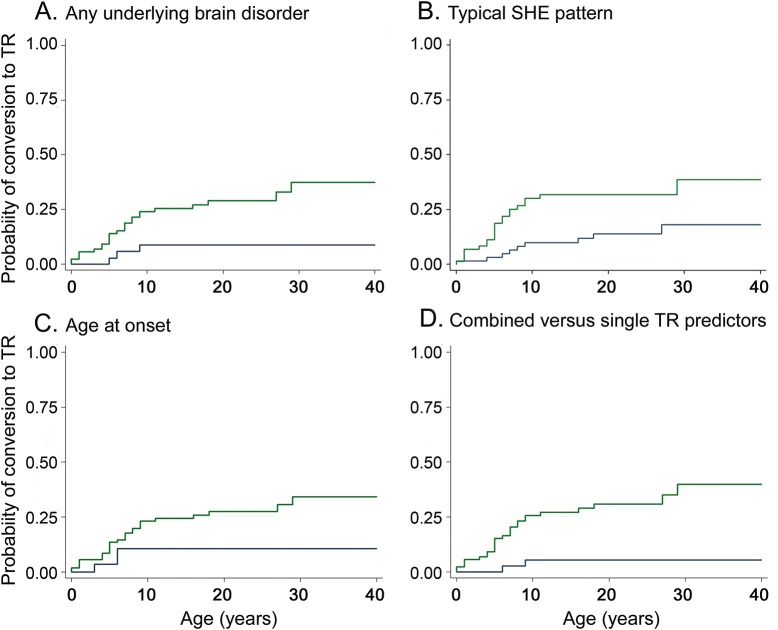
Results: We included 139 patients with a 16-year median follow-up (2,414 person-years). The mean age at onset was 13 ± 10 years. SHE was sporadic in 86% of cases and familial in 14%; 16% of patients had underlying brain abnormalities. Forty-five percent of patients had at least 1 seizure in wakefulness lifetime and 55% had seizures only in sleep (typical SHE). At the last assessment, 31 patients achieved TR (TR group, 22.3%), while 108 (NTR group, 77.7%) still had seizures or had been in remission for <5 years. The cumulative TR rate was 20.4%, 23.5%, and 28.4% by 10, 20, and 30 years from inclusion. At univariate analysis, any underlying brain disorder (any combination of intellectual disability, perinatal insult, pathologic neurologic examination, and brain structural abnormalities) and seizures in wakefulness were more frequent among the NTR group (p = 0.028; p = 0.043). Absence of any underlying brain disorder (hazard ratio 4.21, 95% confidence interval 1.26-14.05, p = 0.020) and typical SHE (hazard ratio 2.76, 95% confidence interval 1.31-5.85, p = 0.008) were associated with TR.
Conclusions: Our data show a poor prognosis of SHE after a long-term follow-up. Its outcome is primarily a function of the underlying etiology.
Copyright © 2016 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Scheffer IE, Bhatia KP, Lopes-Cendes I, et al. . Autosomal dominant nocturnal frontal lobe epilepsy: a distinctive clinical disorder. Brain 1995;118:61–73. - PubMed
-
- Steinlein OK, Hoda JC, Bertrand S, Bertrand D. Mutations in familial nocturnal frontal lobe epilepsy might be associated with distinct neurological phenotypes. Seizure 2012;21:118–123. - PubMed
-
- Heron SE, Smith KR, Bahlo M, et al. . Missense mutations in the sodium-gated potassium channel gene KCNT1 cause severe autosomal dominant nocturnal frontal lobe epilepsy. Nat Genet 2012;44:1188–1190. - PubMed
-
- Provini F, Plazzi G, Tinuper P, Vandi S, Lugaresi E, Montagna P. Nocturnal frontal lobe epilepsy: a clinical and polygraphic overview of 100 consecutive cases. Brain 1999;122:1017–1031. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases