

Diagnostic value of high-frequency ultrasound and magnetic resonance imaging in early rheumatoid arthritis
- PMID: 27882112
- PMCID: PMC5103740
- DOI: 10.3892/etm.2016.3695
Diagnostic value of high-frequency ultrasound and magnetic resonance imaging in early rheumatoid arthritis
Abstract
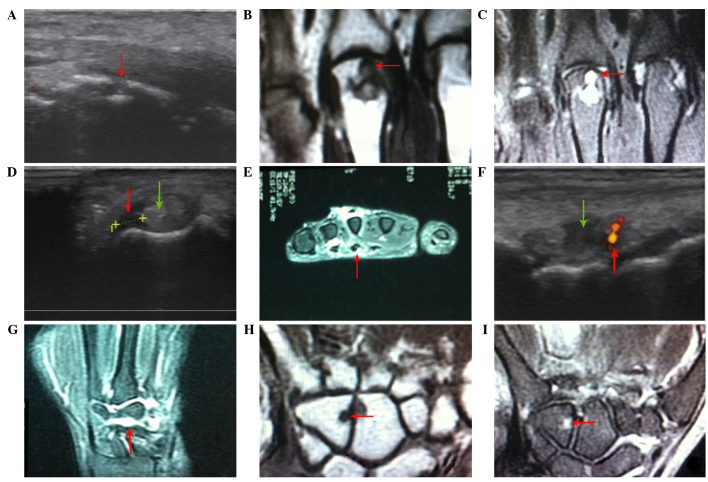
Early diagnosis and management improve the outcome of patients with rheumatoid arthritis (RA). The present study explored the application of high-frequency ultrasound (US) and magnetic resonance imaging (MRI) in the detection of early RA. Thirty-nine patients (20 males and 19 females) diagnosed with early RA were enrolled in the study. A total of 1,248 positions, including 858 hand joints and 390 tendons, were examined by high-frequency US and MRI to evaluate the presence of bone erosion, bone marrow edema (BME), synovial proliferation, joint effusion, tendinitis and tendon sheath edema. The imaging results of the above abnormalities, detected by US, were compared with those identified using MRI. No statistically significant overall changes were observed between high-frequency US and MRI in detecting bone erosion [44 (5.1%) vs. 35 (4.1%), respectively; P>0.05], tendinitis [18 (4.6%) vs. 14 (1.5%), respectively; P>0.05] and tendon sheath edema [37 (9.5%) vs. 30 (7.7%), respectively; P>0.05]. Significant differences were observed between high-frequency US and MRI with regards to the detection of synovial proliferation [132 (15.4%) vs. 66 (7.7%), respectively; P<0.05] and joint effusion [89 (10.4%) vs. 52 (6.1%), respectively; P<0.05]. In addition, significant differences were identified between the detection of BME using MRI compared with high-frequency US (5.5 vs. 0%, respectively; P<0.05). MRI and high-frequency US of the dominant hand and wrist joints were comparably sensitive to bone erosion, tendinitis and tendon sheath edema. However, MRI was more sensitive in detecting bone marrow edema in early RA, while US was more sensitive in the evaluation of joint effusion and synovial proliferation. In conclusion, US and MRI are promising for the detection and diagnosis of inflammatory activity in patients with RA.
Keywords: bone erosion; high frequency ultrasonography; magnetic resonance imaging; rheumatoid arthritis; synovial proliferation.
Figures
Similar articles
-
Bilateral evaluation of the hand and wrist in untreated early inflammatory arthritis: a comparative study of ultrasonography and magnetic resonance imaging.J Rheumatol. 2013 Aug;40(8):1282-92. doi: 10.3899/jrheum.120713. Epub 2013 Jun 1. J Rheumatol. 2013. PMID: 23729806
-
Magnetic resonance imaging-assessed synovial and bone changes in hand and wrist joints of rheumatoid arthritis patients.Korean J Intern Med. 2019 May;34(3):651-659. doi: 10.3904/kjim.2016.271. Epub 2017 Nov 24. Korean J Intern Med. 2019. PMID: 29166759 Free PMC article.
-
Screening for early rheumatoid arthritis using high-frequency ultrasound, serum RANKL, and OPG detection.Clin Rheumatol. 2024 Jan;43(1):159-166. doi: 10.1007/s10067-023-06830-2. Epub 2023 Dec 5. Clin Rheumatol. 2024. PMID: 38051416
-
Diagnostic test accuracy of magnetic resonance imaging and ultrasound for detecting bone erosion in patients with rheumatoid arthritis.Clin Rheumatol. 2020 Apr;39(4):1283-1293. doi: 10.1007/s10067-019-04825-6. Epub 2019 Nov 12. Clin Rheumatol. 2020. PMID: 31713730 Review.
-
Magnetic resonance imaging in early detection of rheumatoid arthritis.Semin Musculoskelet Radiol. 2003 Jun;7(2):79-94. doi: 10.1055/s-2003-41342. Semin Musculoskelet Radiol. 2003. PMID: 12920646 Review.
Cited by
-
Reliability of Ultrasound for the Detection of Rheumatoid Arthritis.J Med Ultrasound. 2019 Jan-Mar;27(1):3-12. doi: 10.4103/JMU.JMU_112_18. Epub 2019 Feb 26. J Med Ultrasound. 2019. PMID: 31031529 Free PMC article. Review.
-
Infrared Thermography and Ultrasonography of the Hands in Rheumatoid Arthritis Patients.J Med Ultrasound. 2021 Jan 9;29(3):212-214. doi: 10.4103/JMU.JMU_113_20. eCollection 2021 Jul-Sep. J Med Ultrasound. 2021. PMID: 34729333 Free PMC article.
-
The Clinical Utility of Musculoskeletal Ultrasound for Disease Activity Evaluation and Therapeutic Response Prediction in Rheumatoid Arthritis Patients: A Narrative Review.J Med Ultrasound. 2023 Nov 10;31(4):275-281. doi: 10.4103/jmu.jmu_126_22. eCollection 2023 Oct-Dec. J Med Ultrasound. 2023. PMID: 38264607 Free PMC article. Review.
-
Musculoskeletal ultrasound as a screening-tool for rheumatoid arthritis: results of the "Rheuma-Truck" screening and awareness initiative.Adv Rheumatol. 2022 Jan 4;62(1):1. doi: 10.1186/s42358-021-00233-0. Adv Rheumatol. 2022. PMID: 34983698
-
Early Undifferentiated Arthritis: A Developing Country Perspective from Nepal.JNMA J Nepal Med Assoc. 2018 Nov-Dec;56(214):983-990. doi: 10.31729/jnma.3893. JNMA J Nepal Med Assoc. 2018. PMID: 31065150 Free PMC article. Review.
References
-
- Gibofsky A. Overview of epidemiology, pathophysiology and diagnosis of rheumatoid arthritis. Am J Manag Care. 2012;18(Suppl 13):S295–S302. - PubMed
-
- Machold KP, Stamm TA, Nell VP, Pflugbeil S, Aletaha D, Steiner G, Uffmann M, Smolen JS. Very recent onset rheumatoid arthritis: Clinical and serological patient characteristics associated with radiographic progression over the first years of disease. Rheumatology (Oxford) 2007;46:342–349. doi: 10.1093/rheumatology/kel237. - DOI - PubMed
-
- Østergaard M, Peterfy C, Conaghan P, McQueen F, Bird P, Ejbjerg B, Shnier R, O'Connor P, Klarlund M, Emery P, et al. OMERACT rheumatoid arthritis magnetic resonance imaging studies. Core set of MRI acquisitions, joint pathology definitions and the OMERACT RA-MRI scoring system. J Rheumatol. 2003;30:1385–1386. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources