A Case of Transverse Myelitis Caused by Varicella Zoster Virus in an Immunocompetent Older Patient
- PMID: 27883372
- PMCID: PMC5204014
- DOI: 10.3947/ic.2016.48.4.334
A Case of Transverse Myelitis Caused by Varicella Zoster Virus in an Immunocompetent Older Patient
Abstract
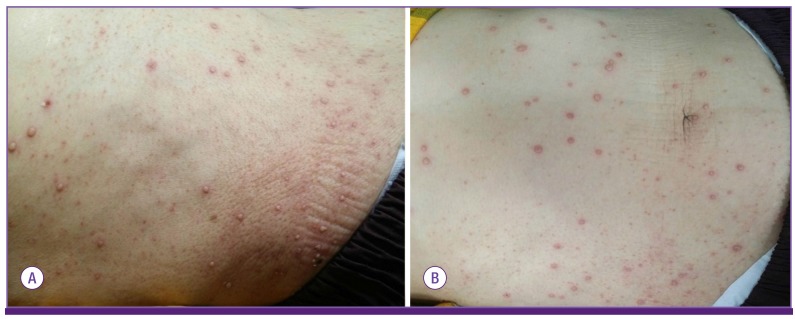
Varicella zoster virus (VZV) is a human neurotropic alphaherpesvirus that causes chickenpox (varicella) in children. VZV reactivation may lead to neurological complications, including transverse myelitis. However, transverse myelitis caused by VZV reactivation is rare in immunocompetent patients. Herein, we report a case of transverse myelitis caused by VZV in an immunocompetent older patient, and confirmed this case by polymerase chain reaction. A 79-year-old woman visited our service with complaints of weakness in the right lower leg, generalized vesicular eruptions, and throbbing pain in the right flank for ten days. Spine MRI showed transverse myelitis in the thoracic spine at level T4-T11. The patient was treated with acyclovir and her neurological functions improved, except for sensory impairment below level T10. For older patients, early and aggressive antiviral treatment against VZV may be necessary even though these patients are immunocompetent.
Keywords: Antiviral treatment; Immunocompetent; Older patients; Transverse myelitis; Varicella zoster virus.
Conflict of interest statement
No conflicts of interest.
Figures

Similar articles
-
Cervical myelitis due to herpes zoster: case report.Postep Psychiatr Neurol. 2022 Dec;31(4):174-177. doi: 10.5114/ppn.2022.125071. Epub 2023 Feb 16. Postep Psychiatr Neurol. 2022. PMID: 37081909 Free PMC article.
-
Transverse myelitis after infection with varicella zoster virus in patient with normal immunity: A case report.World J Clin Cases. 2021 Nov 26;9(33):10308-10314. doi: 10.12998/wjcc.v9.i33.10308. World J Clin Cases. 2021. PMID: 34904104 Free PMC article.
-
[Transverse myelitis and cauda equina syndrome followed by varicella in a patient with varicella-zoster virus infection].Rinsho Shinkeigaku. 2023 Oct 25;63(10):637-642. doi: 10.5692/clinicalneurol.cn-001833. Epub 2023 Sep 30. Rinsho Shinkeigaku. 2023. PMID: 37779026 Japanese.
-
Clinical Features of Varicella-Zoster Virus Infection.Viruses. 2018 Nov 2;10(11):609. doi: 10.3390/v10110609. Viruses. 2018. PMID: 30400213 Free PMC article. Review.
-
The Spectrum of Neurological Manifestations of Varicella-Zoster Virus Reactivation.Viruses. 2023 Jul 30;15(8):1663. doi: 10.3390/v15081663. Viruses. 2023. PMID: 37632006 Free PMC article. Review.
Cited by
-
Transverse myelitis caused by varicella-zoster.BMJ Case Rep. 2021 Aug 30;14(8):e238078. doi: 10.1136/bcr-2020-238078. BMJ Case Rep. 2021. PMID: 34462272 Free PMC article.
-
Detection of varicella-zoster virus from cerebrospinal fluid using advanced fragment analysis in a child with encephalitis: a case report.BMC Infect Dis. 2019 Apr 25;19(1):342. doi: 10.1186/s12879-019-3986-3. BMC Infect Dis. 2019. PMID: 31023250 Free PMC article.
-
Longitudinally Extensive Transverse Myelitis (LETM) Following Varicella Infection in a 13-Year Immunocompetent Child.Iran J Child Neurol. 2019 Winter;13(1):121-126. Iran J Child Neurol. 2019. PMID: 30598680 Free PMC article.
-
Transverse myelitis caused by herpes zoster following COVID-19 vaccination: A case report.World J Clin Cases. 2023 Feb 26;11(6):1419-1425. doi: 10.12998/wjcc.v11.i6.1419. World J Clin Cases. 2023. PMID: 36926132 Free PMC article.
-
Longitudinal Extensive Transverse Myelitis in an Immunocompetent Older Individual-A Rare Complication of Varicella-Zoster Virus Reactivation.Medicina (Kaunas). 2019 May 23;55(5):201. doi: 10.3390/medicina55050201. Medicina (Kaunas). 2019. PMID: 31126152 Free PMC article.
References
-
- Gilden DH, Kleinschmidt-DeMasters BK, LaGuardia JJ, Mahalingam R, Cohrs RJ. Neurologic complications of the reactivation of varicella-zoster virus. N Engl J Med. 2000;342:635–645. - PubMed
-
- Amlie-Lefond C, Jubelt B. Neurologic manifestations of varicella zoster virus infections. Curr Neurol Neurosci Rep. 2009;9:430–434. - PubMed
-
- Hung CH, Chang KH, Kuo HC, Huang CC, Liao MF, Tsai YT, Ro LS. Features of varicella zoster virus myelitis and dependence on immune status. J Neurol Sci. 2012;318:19–24. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials