

Identifying and prioritizing lower value services from Dutch specialist guidelines and a comparison with the UK do-not-do list
- PMID: 27884150
- PMCID: PMC5123317
- DOI: 10.1186/s12916-016-0747-7
Identifying and prioritizing lower value services from Dutch specialist guidelines and a comparison with the UK do-not-do list
Abstract
Background: The term 'lower value services' concerns healthcare that is of little or no value to the patient and consequently should not be provided routinely, or not be provided at all. De-adoption of lower value care may occur through explicit recommendations in clinical guidelines. The present study aimed to generate a comprehensive list of lower value services for the Netherlands that assesses the type of care and associated medical conditions. The list was compared with the NICE do-not-do list (United Kingdom). Finally, the feasibility of prioritizing the list was studied to identify conditions where de-adoption is warranted.
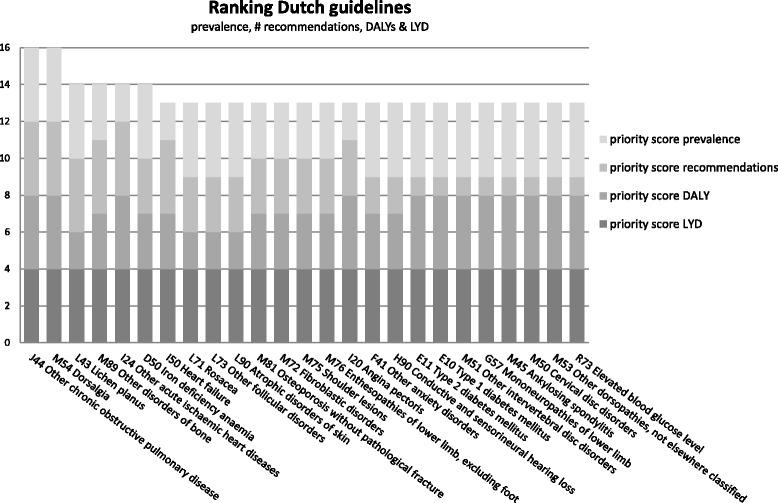
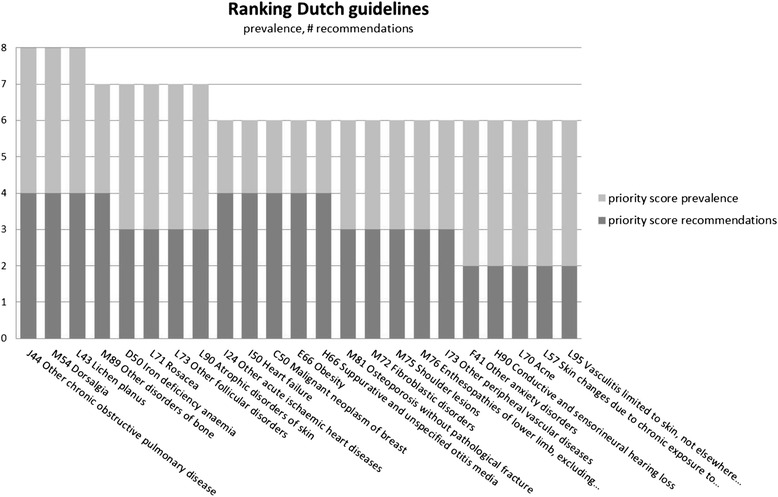
Methods: Dutch clinical guidelines (published from 2010 to 2015) were searched for lower value services. The lower value services identified were categorized by type of care (diagnostics, treatment with and without medication), type of lower value service (not routinely provided or not provided at all), and ICD10 codes (international classification of diseases). The list was prioritized per ICD10 code, based on the number of lower value services per ICD10 code, prevalence, and burden of disease.
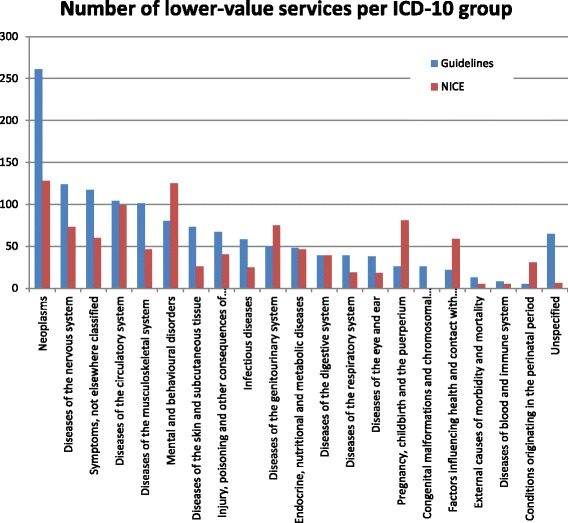
Results: A total of 1366 lower value services were found in the 193 Dutch guidelines included in our study. Of the lower value services, 30% covered diagnostics, 29% related to surgical and medical treatment without drugs primarily, and 39% related to drug treatment. The majority (77%) of all lower value services was on care that should not be offered at all, whereas the other 23% recommended on care that should not be offered routinely. ICD10 chapters that included most lower value services were neoplasms and diseases of the nervous system. Dutch guidelines appear to contain more lower value services than UK guidelines. The prioritization processes revealed several conditions, including back pain, chronic obstructive pulmonary disease, and ischemic heart diseases, where lower value services most likely occur and de-adoption is warranted.
Conclusions: In this study, a comprehensive list of lower value services for Dutch hospital care was developed. A feasible method for prioritizing lower value services was established. Identifying and prioritizing lower value services is the first of several necessary steps in reducing them.
Keywords: Choosing Wisely; De-adoption; De-implementation; Disinvestment; Guideline; Low-value; Medical reversal; Waste.
Figures
Similar articles
-
Identifying and prioritizing do-not-do recommendations in Dutch primary care.BMC Prim Care. 2022 Jun 3;23(1):141. doi: 10.1186/s12875-022-01713-y. BMC Prim Care. 2022. PMID: 35658832 Free PMC article.
-
Low-value and high-value care recommendations in nursing: A systematic assessment of clinical practice guidelines.J Nurs Scholarsh. 2025 May;57(3):486-499. doi: 10.1111/jnu.13029. Epub 2024 Nov 20. J Nurs Scholarsh. 2025. PMID: 39567352 Free PMC article. Review.
-
Moving low value care lists into action: prioritizing candidate health technologies for reassessment using administrative data.BMC Health Serv Res. 2018 Aug 15;18(1):640. doi: 10.1186/s12913-018-3459-1. BMC Health Serv Res. 2018. PMID: 30111308 Free PMC article.
-
Low-value care in nursing: A systematic assessment of clinical practice guidelines.Int J Nurs Stud. 2018 Nov;87:34-39. doi: 10.1016/j.ijnurstu.2018.07.002. Epub 2018 Jul 6. Int J Nurs Stud. 2018. PMID: 30053680
-
The UK model for system redesign and chronic kidney disease services.Semin Nephrol. 2009 Sep;29(5):475-82. doi: 10.1016/j.semnephrol.2009.06.004. Semin Nephrol. 2009. PMID: 19751892 Review.
Cited by
-
Evaluation of bottom-up interventions targeting community-dwelling frail older people in Belgium: methodological challenges and lessons for future comparative effectiveness studies.BMC Health Serv Res. 2019 Jun 24;19(1):416. doi: 10.1186/s12913-019-4240-9. BMC Health Serv Res. 2019. PMID: 31234857 Free PMC article.
-
Factors influencing current low-value follow-up care after basal cell carcinoma and suggested strategies for de-adoption: a qualitative study.Br J Dermatol. 2019 Jun;180(6):1420-1429. doi: 10.1111/bjd.17594. Epub 2019 Mar 28. Br J Dermatol. 2019. PMID: 30597525 Free PMC article.
-
Assessing volume and variation of low-value care practices in the Netherlands.Eur J Public Health. 2020 Apr 1;30(2):236-240. doi: 10.1093/eurpub/ckz245. Eur J Public Health. 2020. PMID: 31950995 Free PMC article.
-
Understanding the public's role in reducing low-value care: a scoping review.Implement Sci. 2020 Apr 7;15(1):20. doi: 10.1186/s13012-020-00986-0. Implement Sci. 2020. PMID: 32264926 Free PMC article.
-
Identifying and prioritizing do-not-do recommendations in Dutch primary care.BMC Prim Care. 2022 Jun 3;23(1):141. doi: 10.1186/s12875-022-01713-y. BMC Prim Care. 2022. PMID: 35658832 Free PMC article.
References
-
- Institute of Medicine. IOM definition of quality. 2001. http://iom.nationalacademies.org/Global/News%20Announcements/Crossing-th.... Accessed 6 June 2016.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
