

CKD and Risk for Hospitalization With Infection: The Atherosclerosis Risk in Communities (ARIC) Study
- PMID: 27884474
- PMCID: PMC5438909
- DOI: 10.1053/j.ajkd.2016.09.018
CKD and Risk for Hospitalization With Infection: The Atherosclerosis Risk in Communities (ARIC) Study
Abstract
Background: Individuals on dialysis therapy have a high risk for infection, but risk for infection in earlier stages of chronic kidney disease has not been comprehensively described.
Study design: Observational cohort study.
Setting & participants: 9,697 participants (aged 53-75 years) in the Atherosclerosis Risk in Communities (ARIC) Study. Participants were followed up from 1996 to 1998 through 2011.
Predictors: Estimated glomerular filtration rate (eGFR) and urinary albumin-creatinine ratio (ACR).
Outcomes: Risk for hospitalization with infection and death during or within 30 days of hospitalization with infection.
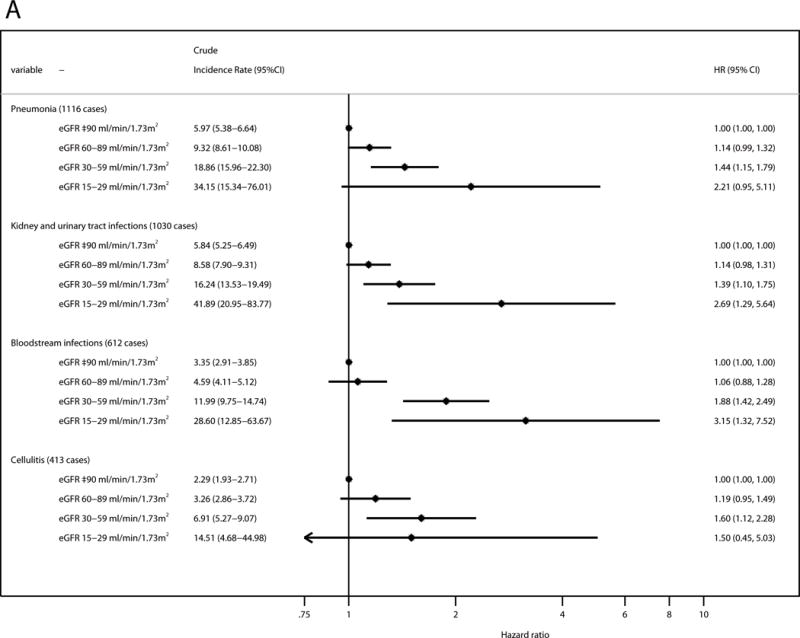
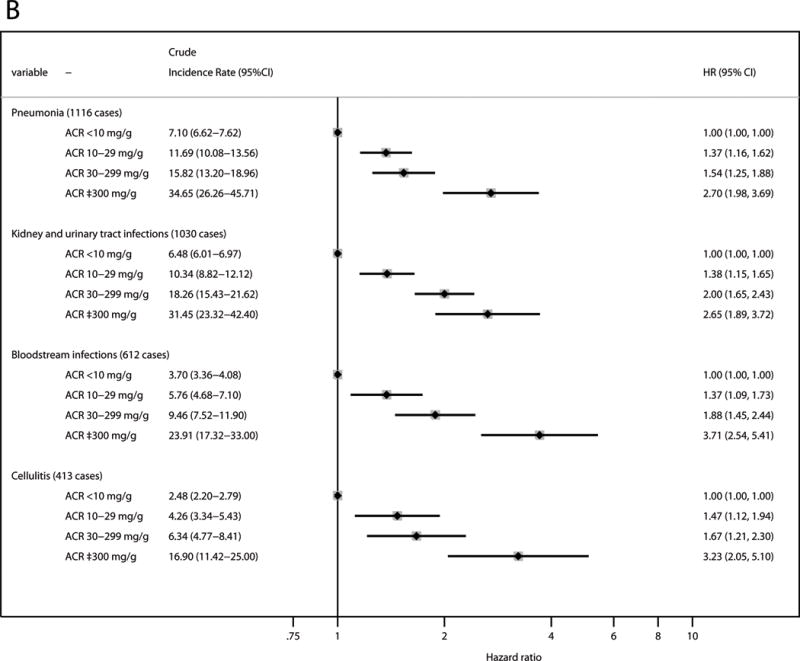
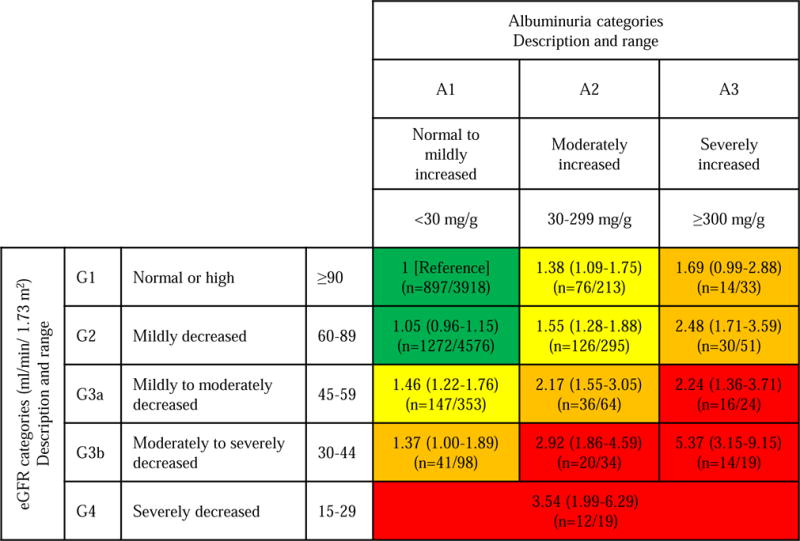
Results: During follow-up (median, 13.6 years), there were 2,701 incident hospitalizations with infection (incidence rate, 23.6/1,000 person-years) and 523 infection-related deaths. In multivariable analysis, HRs of incident hospitalization with infection as compared to eGFRs≥90mL/min/1.73m2 were 2.55 (95% CI, 1.43-4.55), 1.48 (95% CI, 1.28-1.71), and 1.07 (95% CI, 0.98-1.16) for eGFRs of 15 to 29, 30 to 59, and 60 to 89mL/min/1.73m2, respectively. Corresponding HRs were 3.76 (95% CI, 1.48-9.58), 1.62 (95% CI, 1.20-2.19), and 0.99 (95% CI, 0.80-1.21) for infection-related death. Compared to ACRs<10mg/g, HRs of incident hospitalization with infection were 2.30 (95% CI, 1.81-2.91), 1.56 (95% CI, 1.36-1.78), and 1.34 (95% CI, 1.20-1.50) for ACRs≥300, 30 to 299, and 10 to 29mg/g, respectively. Corresponding HRs were 3.44 (95% CI, 2.28-5.19), 1.57 (95% CI, 1.18-2.09), and 1.39 (95% CI, 1.09-1.78) for infection-related death. Results were consistent when separately assessing risk for pneumonia, kidney and urinary tract infections, bloodstream infections, and cellulitis and when taking into account recurrent episodes of infection.
Limitations: Outcome ascertainment relied on diagnostic codes at time of discharge.
Conclusions: Increasing provider awareness of chronic kidney disease as a risk factor for infection is needed to reduce infection-related morbidity and mortality.
Keywords: Chronic kidney disease (CKD); albuminuria; bacteremia; cellulitis; chronic kidney failure; chronic renal insufficiency; glomerular filtration rate (GFR); hospitalization; infection; infectious disease; kidney function; pneumonia; proteinuria; respiratory tract infections; urinary tract infections.
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Kidney Disease Statistics for the United States. Available: http://www.niddk.nih.gov/health-information/health-statistics/Pages/kidn.... Accessed 3 Feb 2016.
-
- Berman SJ, Johnson EW, Nakatsu C, Alkan M, Chen R, LeDuc J. Burden of infection in patients with end-stage renal disease requiring long-term dialysis. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2004;39:1747–1753. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- K23 DK106515/DK/NIDDK NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- R01 DK100446/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
