

Frailty, Kidney Function, and Polypharmacy: The Atherosclerosis Risk in Communities (ARIC) Study
- PMID: 27884475
- PMCID: PMC5263025
- DOI: 10.1053/j.ajkd.2016.08.034
Frailty, Kidney Function, and Polypharmacy: The Atherosclerosis Risk in Communities (ARIC) Study
Abstract
Background: Frail individuals are at increased risk for poor outcomes, including adverse drug events. Kidney function is often compromised in frailty and is a key consideration in medication choice and dosing; however, creatinine-based measures of kidney function may be biased in frail individuals.
Study design: Observational study.
Setting & participants: 4,987 community-dwelling older men and women with complete data who participated in visit 5 of the Atherosclerosis Risk in Communities (ARIC) Study (2011-2013).
Predictors: Kidney measures included glomerular filtration rate (GFR) estimated using serum creatinine (eGFRcr) and serum cystatin C level (eGFRcys) and urine albumin-creatinine ratio.
Outcome: Frailty, defined using established criteria of 3 or more frailty characteristics (weight loss, slowness, exhaustion, weakness, and low physical activity).
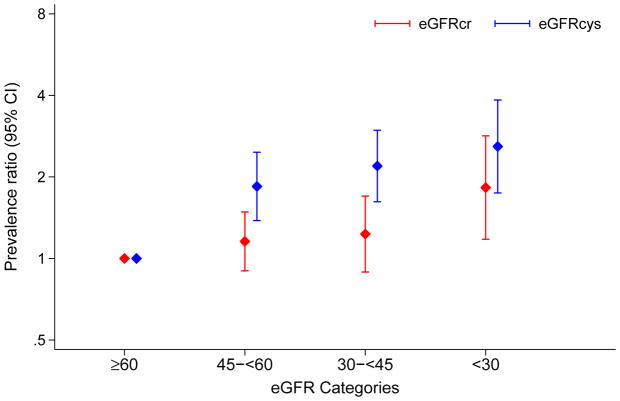
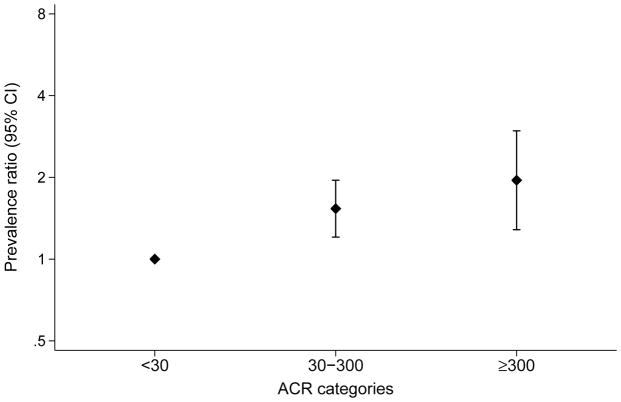
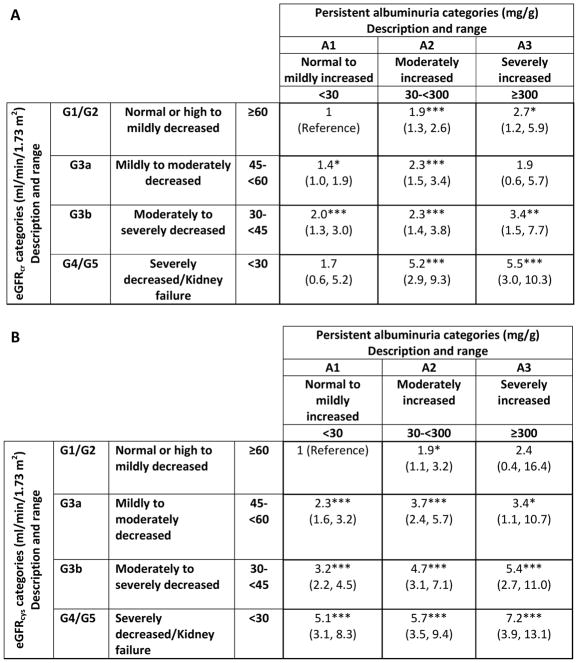
Results: 341 (7%) participants were classified as frail, 1,475 (30%) had eGFRcr<60mL/min/1.73m2, 2,480 (50%) had eGFRcys<60mL/min/1.73m2, and 1,006 (20%) had albuminuria with albumin excretion ≥ 30mg/g. Among frail participants, prevalences of eGFRcr and eGFRcys<60mL/min/1.73m2 were 45% and 77%, respectively. Adjusted for covariates, frailty showed a moderate association with eGFRcr and a strong association with eGFRcys and albumin-creatinine ratio. Frail individuals with eGFRcr of 60 to <75mL/min/1.73m2 were frequently reclassified to lower eGFR categories using eGFRcys (49% to 45-<60, 32% to 30-<45, and 3% to <30mL/min/1.73m2). Hyperpolypharmacy (taking ≥10 classes of medications) was more common in frail individuals (54% vs 38% of nonfrail), including classes requiring kidney clearance (eg, digoxin) and associated with falls and subsequent complications (eg, hypnotic/sedatives and anticoagulants).
Limitations: Cross-sectional study design.
Conclusions: Frail individuals had a high prevalence of reduced kidney function, with large discrepancies when reduced kidney function was classified by eGFRcys versus eGFRcr. Given the substantial medication burden and uncertainty in chronic kidney disease classification, confirmation of kidney function with alternative biomarkers may be warranted to ensure careful prescribing practices in this vulnerable population.
Keywords: Frailty; albuminuria; biomarker; chronic kidney disease (CKD); estimated glomerular filtration rate (eGFR); frail; geriatric; older adults; polypharmacy; prefrail; reduced kidney function; serum creatinine; serum cystatin C; urine albumin.
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. The journals of gerontology. Series A, Biological sciences and medical sciences. 2001;56(3):M146–156. - PubMed
-
- Zaslavsky O, Cochrane BB, Thompson HJ, Woods NF, Herting JR, LaCroix A. Frailty: a review of the first decade of research. Biological research for nursing. 2013;15(4):422–432. - PubMed
-
- Shamliyan T, Talley KM, Ramakrishnan R, Kane RL. Association of frailty with survival: a systematic literature review. Ageing research reviews. 2013;12(2):719–736. - PubMed
-
- Hubbard RE, O’Mahony MS, Woodhouse KW. Medication prescribing in frail older people. European journal of clinical pharmacology. 2013;69(3):319–326. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- R01 DK089174/DK/NIDDK NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- N01 HC055019/HC/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- U01 HL096814/HL/NHLBI NIH HHS/United States
- K08 DK092287/DK/NIDDK NIH HHS/United States
- R01 DK100446/DK/NIDDK NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- K01 AG043501/AG/NIA NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- K24 DK106414/DK/NIDDK NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- R01 HL070825/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- U01 HL096899/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
