

Traumatic brain injury in England and Wales: prospective audit of epidemiology, complications and standardised mortality
- PMID: 27884843
- PMCID: PMC5168492
- DOI: 10.1136/bmjopen-2016-012197
Traumatic brain injury in England and Wales: prospective audit of epidemiology, complications and standardised mortality
Abstract
Objectives: To provide a comprehensive assessment of the management of traumatic brain injury (TBI) relating to epidemiology, complications and standardised mortality across specialist units.
Design: The Trauma Audit and Research Network collects data prospectively on patients suffering trauma across England and Wales. We analysed all data collected on patients with TBI between April 2014 and June 2015.
Setting: Data were collected on patients presenting to emergency departments across 187 hospitals including 26 with specialist neurosurgical services, incorporating factors previously identified in the Ps14 multivariate logistic regression (Ps14n) model multivariate TBI outcome prediction model. The frequency and timing of secondary transfer to neurosurgical centres was assessed.
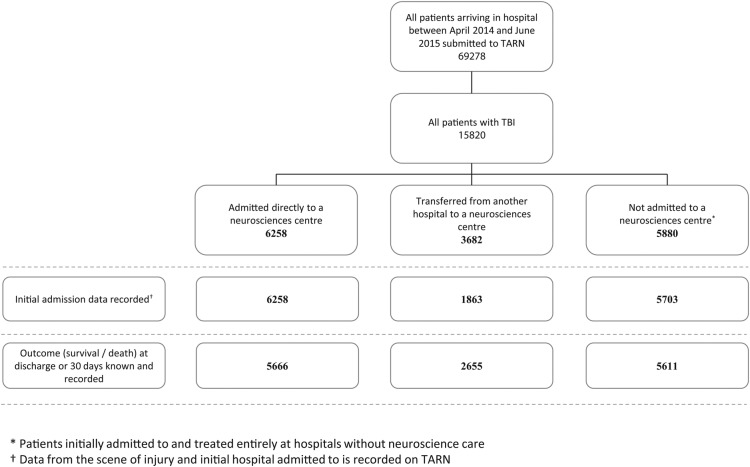
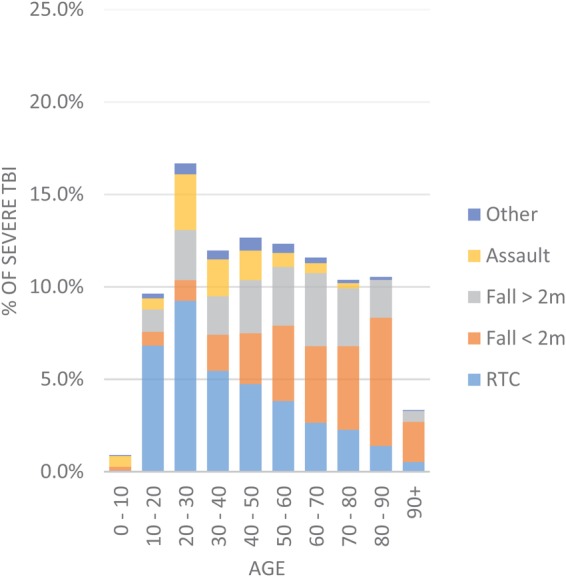
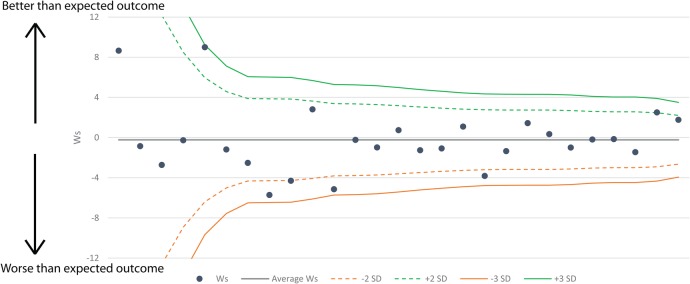
Results: We identified 15 820 patients with TBI presenting to neurosurgical centres directly (6258), transferred from a district hospital to a neurosurgical centre (3682) and remaining in a district general hospital (5880). The commonest mechanisms of injury were falls in the elderly and road traffic collisions in the young, which were more likely to present in coma. In severe TBI (Glasgow Coma Score (GCS) ≤8), the median time from admission to imaging with CT scan is 0.5 hours. Median time to craniotomy from admission is 2.6 hours and median time to intracranial pressure monitoring is 3 hours. The most frequently documented complication of severe TBI is bronchopneumonia in 5% of patients. Risk-adjusted W scores derived from the Ps14n model indicate that no neurosurgical unit fell outside the 3 SD limits on a funnel plot.
Conclusions: We provide the first comprehensive report of the management of TBI in England and Wales, including data from all neurosurgical units. These data provide transparency and suggests equity of access to high-quality TBI management provided in England and Wales.
Keywords: ACCIDENT & EMERGENCY MEDICINE; NEUROSURGERY; TRAUMA MANAGEMENT.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures

References
-
- National Institute for Health and Clinical Excellence: Guidance. Head injury: triage, assessment, investigation and early management of head injury in children, young people and adults. London: National Institute for Health and Care Excellence (UK), 2014. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous