

Sex based subgroup differences in randomized controlled trials: empirical evidence from Cochrane meta-analyses
- PMID: 27884869
- PMCID: PMC5122320
- DOI: 10.1136/bmj.i5826
Sex based subgroup differences in randomized controlled trials: empirical evidence from Cochrane meta-analyses
Abstract
Objective: To evaluate the frequency, validity, and relevance of statistically significant (P<0.05) sex-treatment interactions in randomized controlled trials in Cochrane meta-analyses.
Design: Meta-epidemiological study.
Data sources: Cochrane Database of Systematic Reviews (CDSR) and PubMed.
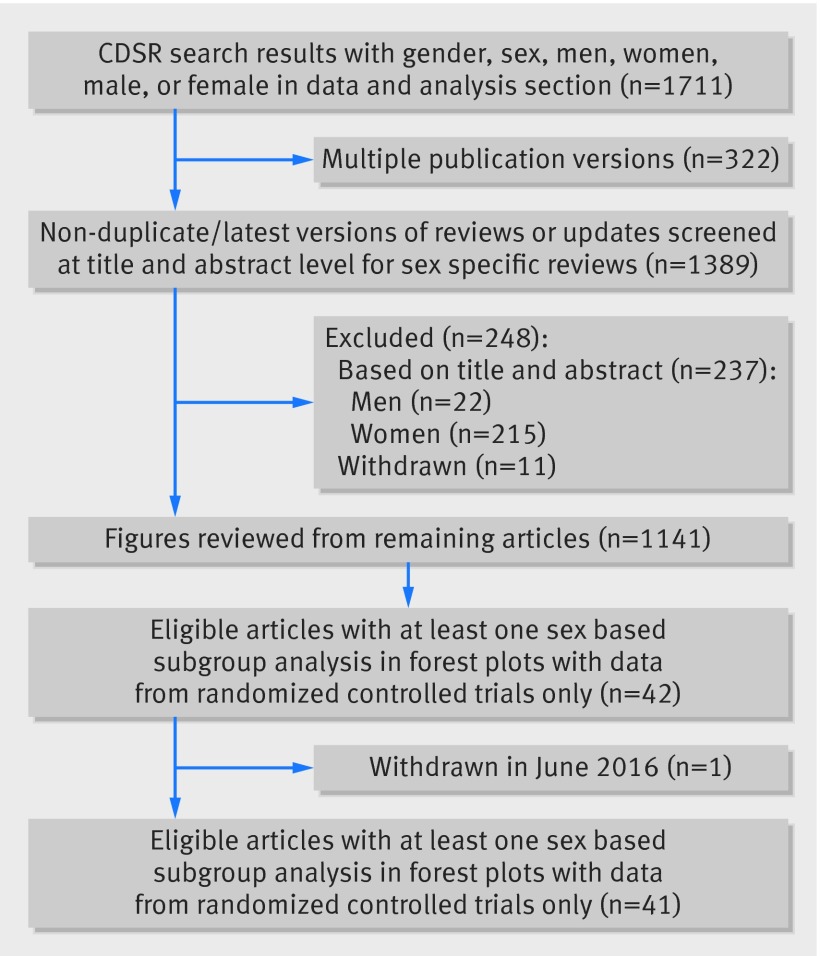
Eligibility criteria for study selection: Reviews published in the CDSR with sex-treatment subgroup analyses in the forest plots, using data from randomized controlled trials.
Data extraction: Information on the study design and sex subgroup data were extracted from reviews and forest plots that met inclusion criteria. For each statistically significant sex-treatment interaction, the potential for biological plausibility and clinical significance was considered.
Results: Among the 41 reviews with relevant data, there were 109 separate treatment-outcome analyses ("topics"). Among the 109 topics, eight (7%) had a statistically significant sex-treatment interaction. The 109 topics included 311 randomized controlled trials (162 with both sexes, 46 with males only, 103 with females only). Of the 162 individual randomized controlled trials that included both sexes, 15 (9%) had a statistically significant sex-treatment interaction. Of four topics where the first published randomized controlled trial had a statistically significant sex-treatment interaction, no meta-analyses that included other randomized controlled trials retained the statistical significance and no meta-analyses showed statistical significance when data from the first published randomized controlled trial were excluded. Of the eight statistically significant sex-treatment interactions from the overall analyses, only three were discussed by the CDSR reviewers for a potential impact on different clinical management for males compared with females. None of these topics had a sex-treatment interaction that influenced treatment recommendations in recent guidelines. UpToDate, an online physician-authored clinical decision support resource, suggested differential management of men and women for one of these sex-treatment interactions.
Conclusion: Statistically significant sex-treatment interactions are only slightly more frequent than what would be expected by chance and there is little evidence of subsequent corroboration or clinical relevance of sex-treatment interactions.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: METRICS (Meta-Research Innovation Center at Stanford) is supported by a grant from the Laura and John Arnold Foundation, PGS received support from the Stanford Clinical and Translational Science Award to Spectrum (NIH UL1 TR 001085), JFT is supported by the NIH (T32 HL007034), EWS is partly supported by the NIH (PRICES project, U01 NS086294), and JPAI is supported by an unrestricted gift by Sue and Bob O’Donnell to Stanford Prevention Research Center; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Sex can affect participation, engagement, and adherence in trials.BMJ. 2016 Dec 30;355:i6754. doi: 10.1136/bmj.i6754. BMJ. 2016. PMID: 28039151 No abstract available.
References
-
- Assmann SF, Pocock SJ, Enos LE, Kasten LE. Subgroup analysis and other (mis)uses of baseline data in clinical trials. Lancet 2000;355:1064-9. 10.1016/S0140-6736(00)02039-0 pmid:10744093. - DOI - PubMed
-
- Bhandari M, Devereaux PJ, Li P, et al. Misuse of baseline comparison tests and subgroup analyses in surgical trials. Clin Orthop Relat Res 2006;447:247-51. 10.1097/01.blo.0000218736.23506.fe pmid:16672904. - DOI - PubMed
-
- Hernández AV, Boersma E, Murray GD, Habbema JD, Steyerberg EW. Subgroup analyses in therapeutic cardiovascular clinical trials: are most of them misleading?Am Heart J 2006;151:257-64. 10.1016/j.ahj.2005.04.020 pmid:16442886. - DOI - PubMed
-
- Pocock SJ, Hughes MD, Lee RJ. Statistical problems in the reporting of clinical trials. A survey of three medical journals. N Engl J Med 1987;317:426-32. 10.1056/NEJM198708133170706 pmid:3614286. - DOI - PubMed
-
- Wang R, Lagakos SW, Ware JH, Hunter DJ, Drazen JM. Statistics in medicine--reporting of subgroup analyses in clinical trials. N Engl J Med 2007;357:2189-94. 10.1056/NEJMsr077003 pmid:18032770. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous