

Comparison of 3 Different Types of Spinal Arteriovenous Shunts below the Conus in Clinical Presentation, Radiologic Findings, and Outcomes
- PMID: 27884878
- PMCID: PMC7963840
- DOI: 10.3174/ajnr.A5001
Comparison of 3 Different Types of Spinal Arteriovenous Shunts below the Conus in Clinical Presentation, Radiologic Findings, and Outcomes
Abstract
Background and purpose: Spinal arteriovenous shunts below the conus constitute 3 types of lesions, which have previously been mainly described in case reports, given their rarity, and are sometimes misdiagnosed. The purpose of this study was to describe the features of each type and compare these types as to epidemiologic features, clinical and radiologic presentations, treatment, and outcomes in a consecutive series of 48 cases.
Materials and methods: The prospectively collected data bases of 2 referral centers for spinal vascular lesions were retrospectively reviewed. Spinal arteriovenous shunts below the conus were defined as all dural and intradural shunts below the conus medullaris. Clinical features, radiologic findings, treatment results, and clinical outcomes were assessed.
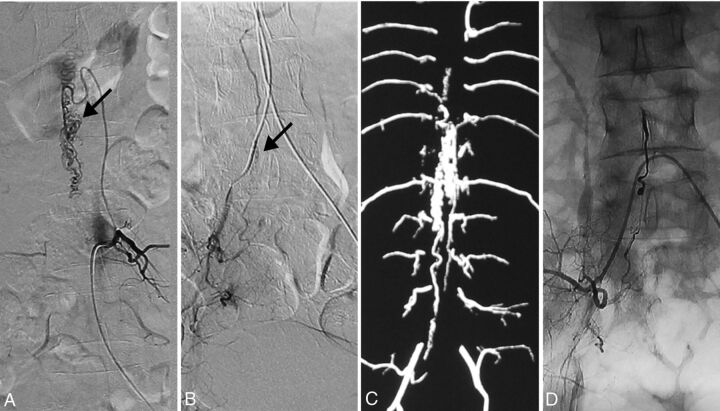
Results: There were filum terminale arteriovenous fistulas in 11 patients (22.9%), radicular arteriovenous shunts in 7 patients (14.6%), and spinal dural arteriovenous fistulas in 30 patients (62.5%). Radicular arteriovenous shunts presented at a younger age (P = .017) and with a higher incidence of back pain symptoms (P = .037). A tethered spinal cord was found in 54.5% of patients with filum terminale arteriovenous fistulas and 23.3% of patients with spinal dural arteriovenous fistulas. After treatment, the angiographic complete obliteration rate was 89.4% and spinal function was improved significantly (P < .001).
Conclusions: Three groups of spinal arteriovenous shunts below the conus can be differentiated according to clinical and radiologic features. Filum terminale arteriovenous fistulas are frequently associated with dysraphic malformations, which may suggest a particular embryologic origin.
© 2017 by American Journal of Neuroradiology.
Figures


References
-
- Rodesch G, Hurth M, Alvarez H, et al. . Angio-architecture of spinal cord arteriovenous shunts at presentation: clinical correlations in adults and children—the Bicêtre experience on 155 consecutive patients seen between 1981–1999. Acta Neurochir (Wien) 2004;146:217–26; discussion 217–226 10.1007/s00701-003-0192-1 - DOI - PubMed
-
- Spetzler RF, Detwiler PW, Riina HA, et al. . Modified classification of spinal cord vascular lesions. J Neurosurg 2002;96:145–56 - PubMed
-
- Lasjaunias P. Spinal cord vascular lesions. J Neurosurg 2003;98(1 suppl):117–19; author reply 119–20 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources