

Odor Identification Screening Improves Diagnostic Classification in Incipient Alzheimer's Disease
- PMID: 27886011
- PMCID: PMC5350629
- DOI: 10.3233/JAD-160842
Odor Identification Screening Improves Diagnostic Classification in Incipient Alzheimer's Disease
Abstract
Background: Measurements of olfaction may serve as useful biomarkers of incipient dementia. Here we examine the improvement in diagnostic accuracy of Alzheimer's disease (AD) and mild cognitive impairment (MCI) when assessing both cognitive functioning and odor identification.
Objective: To determine the utility of odor identification as a supplementary screening test in incipient AD.
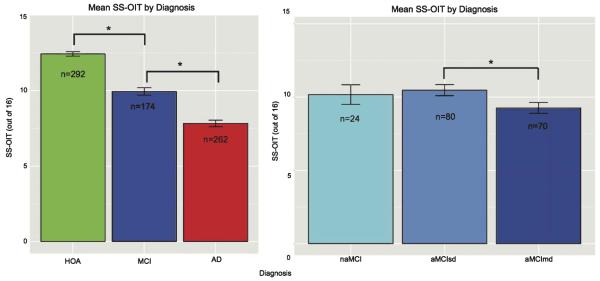
Methods: Sniffin' Sticks Odor Identification Test (SS-OIT) and the Montreal Cognitive Assessment (MoCA) were administered in 262 AD, 174 MCI [150 amnestic (aMCI), and 24 non-amnestic (naMCI)], and 292 healthy older adults (HOA).
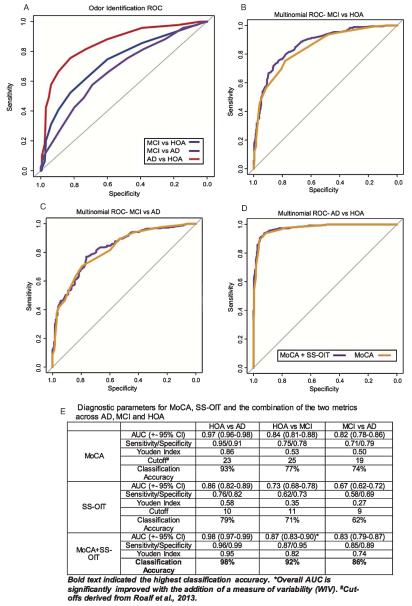
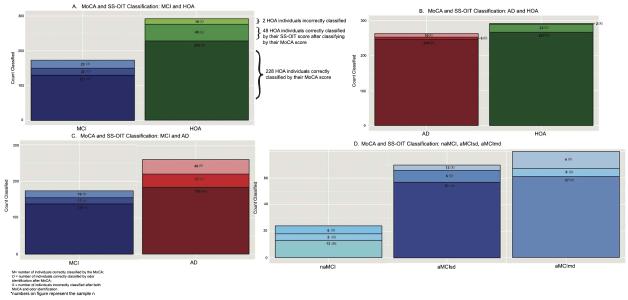
Results: Odor identification scores were higher in HOA relative to MCI or AD groups, and MCI outperformed AD. Odor identification scores were higher in aMCI single domain than aMCI multiple domain. Complementing MoCA scores with the SS-OIT significantly improved diagnostic accuracy of individuals with AD and MCI, including within MCI subgroups.
Discussion: Odor identification is a useful supplementary screening tool that provides additional information relevant for clinical categorization of AD and MCI, including those who are at highest risk to convert to AD.
Keywords: Alzheimer’s disease; Montreal Cognitive Assessment; Sniffin’ Sticks Olfactory Identification Test; mild cognitive impairment; odor identification; smell.
Figures

References
-
- Conti MZ, Vicini-Chilovi B, Riva M, Zanetti M, Liberini P, Padovani A, Rozzini L. Odor identification deficit predicts clinical conversion from mild cognitive impairment to dementia due to Alzheimer’s disease. Arch Clin Neuropsychol. 2013;28:391–399. - PubMed
-
- Petersen RC, Stevens JC, Ganguli M, Tangalos EG, Cummings JL, DeKosky ST. Practice parameter: Early detection of dementia: Mild cognitive impairment (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56:1133–1142. - PubMed
-
- Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L, Wahlund LO, Nordberg A, Backman L, Albert M, Almkvist O, Arai H, Basun H, Blennow K, de Leon M, DeCarli C, Erkinjuntti T, Giacobini E, Graff C, Hardy J, Jack C, Jorm A, Ritchie K, van Duijn C, Visser P, Petersen RC. Mild cognitive impairment–beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J Intern Med. 2004;256:240–246. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
