

Pelvic floor dynamics during high-impact athletic activities: A computational modeling study
- PMID: 27886590
- PMCID: PMC5519824
- DOI: 10.1016/j.clinbiomech.2016.11.003
Pelvic floor dynamics during high-impact athletic activities: A computational modeling study
Abstract
Background: Stress urinary incontinence is a significant problem in young female athletes, but the pathophysiology remains unclear because of the limited knowledge of the pelvic floor support function and limited capability of currently available assessment tools. The aim of our study is to develop an advanced computer modeling tool to better understand the dynamics of the internal pelvic floor during highly transient athletic activities.
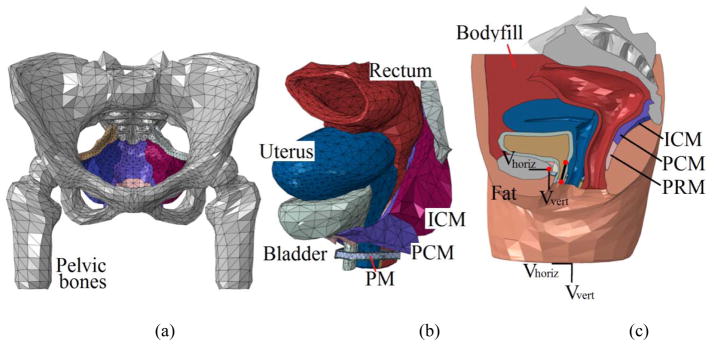
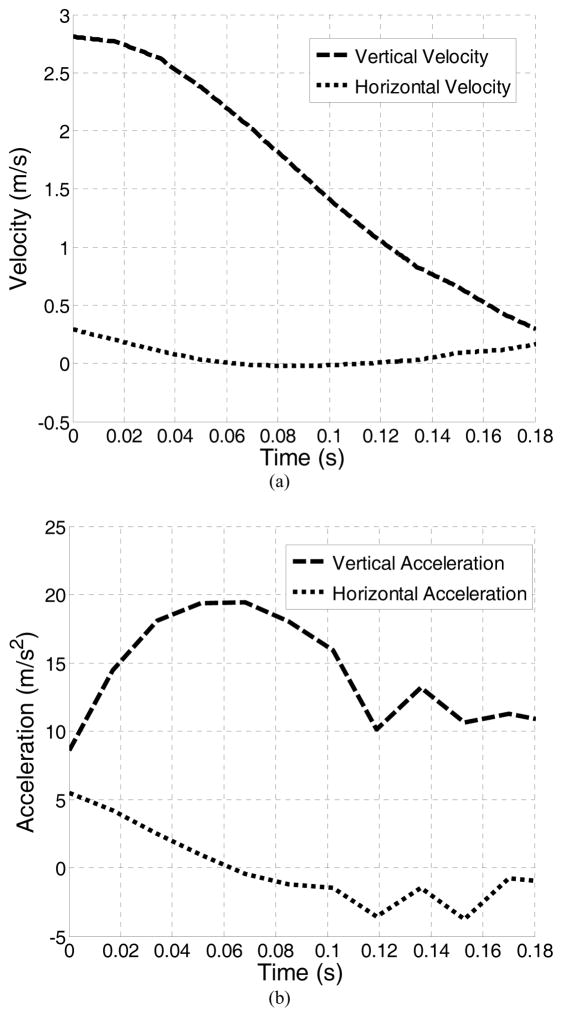
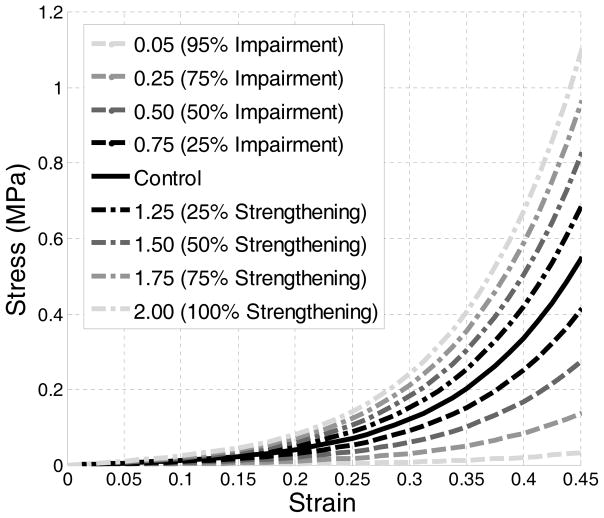
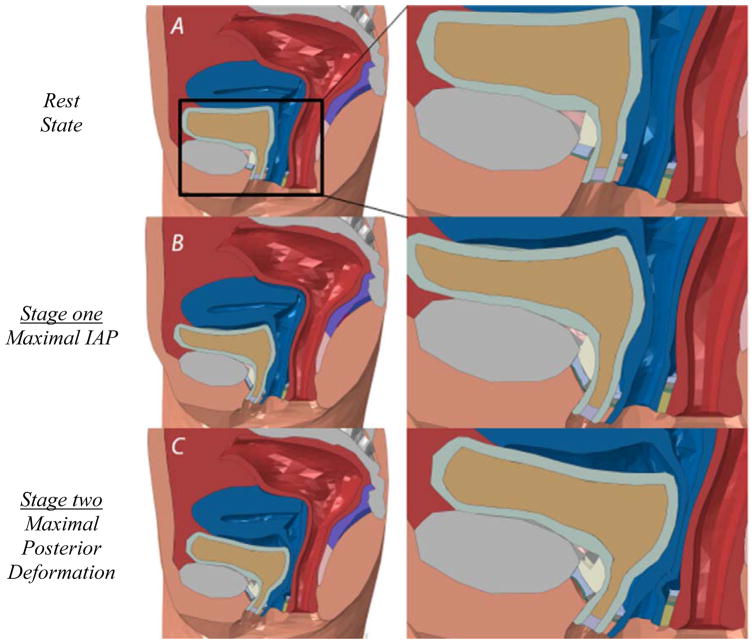
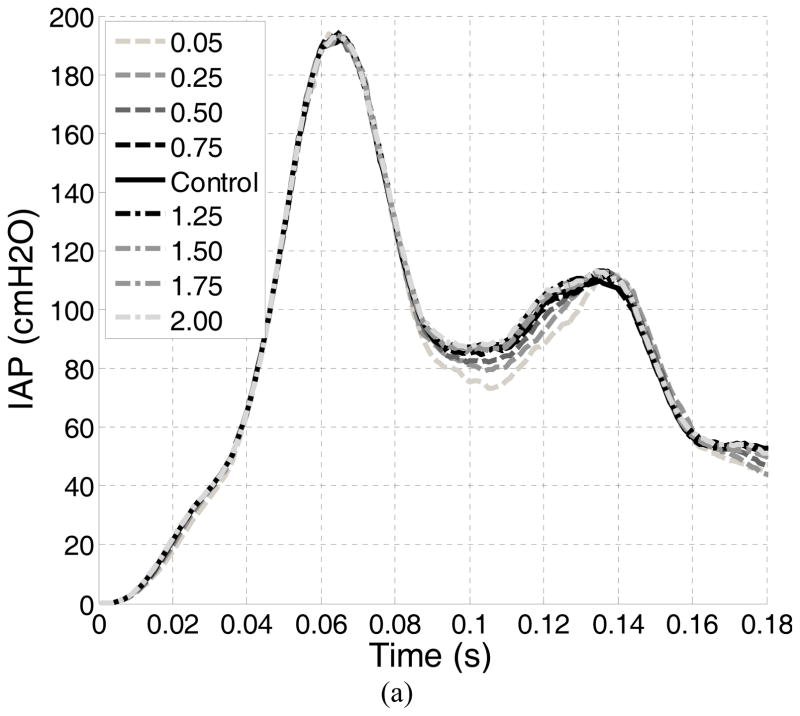
Methods: Apelvic model was developed based on high-resolution MRI scans of a healthy nulliparous young female. A jump-landing process was simulated using realistic boundary conditions captured from jumping experiments. Hypothesized alterations of the function of pelvic floor muscles were simulated by weakening or strengthening the levator ani muscle stiffness at different levels. Intra-abdominal pressures and corresponding deformations of pelvic floor structures were monitored at different levels of weakness or enhancement.
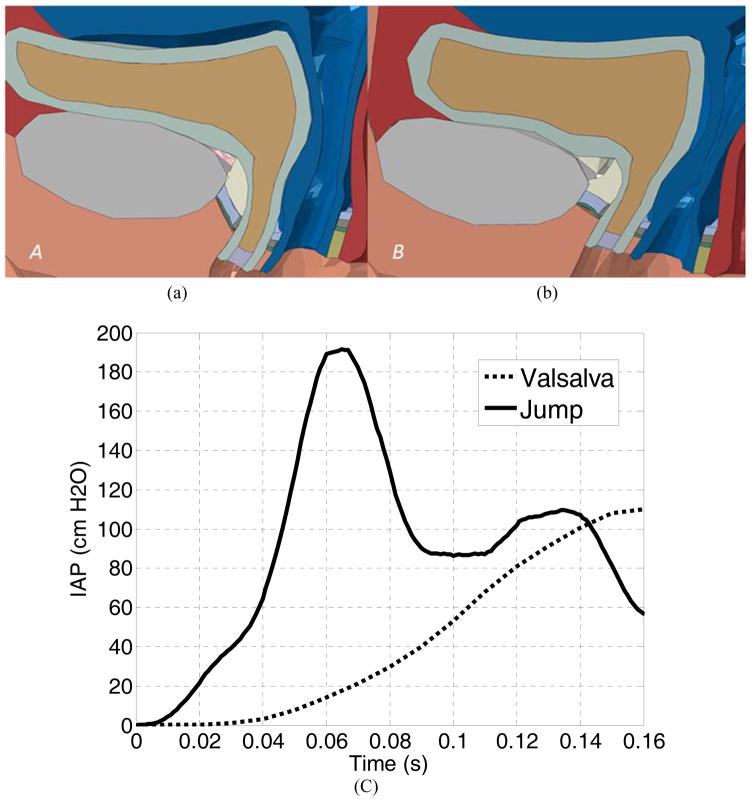
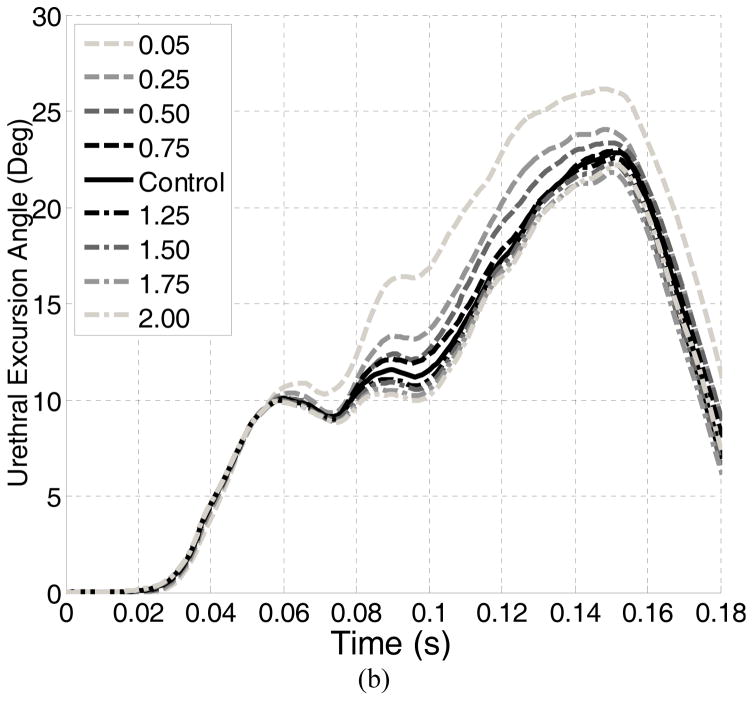
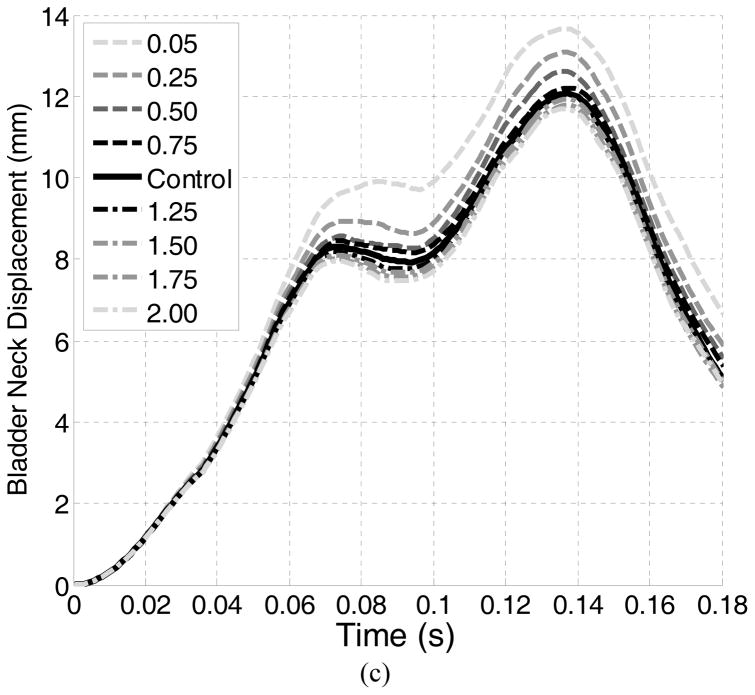
Findings: Results show that pelvic floor deformations generated during a jump-landing process differed greatly from those seen in a Valsalva maneuver which is commonly used for diagnosis in clinic. The urethral mobility was only slightly influenced by the alterations of the levator ani muscle stiffness. Implications for risk factors and treatment strategies were also discussed.
Interpretation: Results suggest that clinical diagnosis should make allowances for observed differences in pelvic floor deformations between a Valsalva maneuver and a jump-landing process to ensure accuracy. Urethral hypermobility may be a less contributing factor than the intrinsic sphincteric closure system to the incontinence of young female athletes.
Keywords: Female athletes; Finite element method; Pelvic floor muscle; Stress urinary incontinence; Urethral hypermobility.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- Almousa S, Moser H, Kitsoulis G, Almousa N, Tzovaras H, Kastani D. The prevalence of urine incontinence in nulliparous female athletes: a systematic review. Physiotherapy. 2015;101:e58.
-
- Hägglund D, Wadensten B. Fear of humiliation inhibits women’s care-seeking behaviour for long-term urinary incontinence. Scandinavian journal of caring sciences. 2007;21(3):305–312. - PubMed
-
- Salvatore S, Serati M, Laterza R, Uccella S, Torella M, Bolis P. The impact of urinary stress incontinence in young and middle-age women practising recreational sports activity: an epidemiological study. British journal of sports medicine. 2009;43(14):1115–1118. - PubMed
-
- DeLancey JO. Structural support of the urethra as it relates to stress urinary incontinence: the hammock hypothesis. American journal of obstetrics and gynecology. 1994;170(6):1713–1723. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
