

Ensuring Patient-Centered Access to Cardiovascular Disease Medicines in Low-Income and Middle-Income Countries Through Health-System Strengthening
- PMID: 27886782
- PMCID: PMC9771684
- DOI: 10.1016/j.ccl.2016.08.008
Ensuring Patient-Centered Access to Cardiovascular Disease Medicines in Low-Income and Middle-Income Countries Through Health-System Strengthening
Abstract
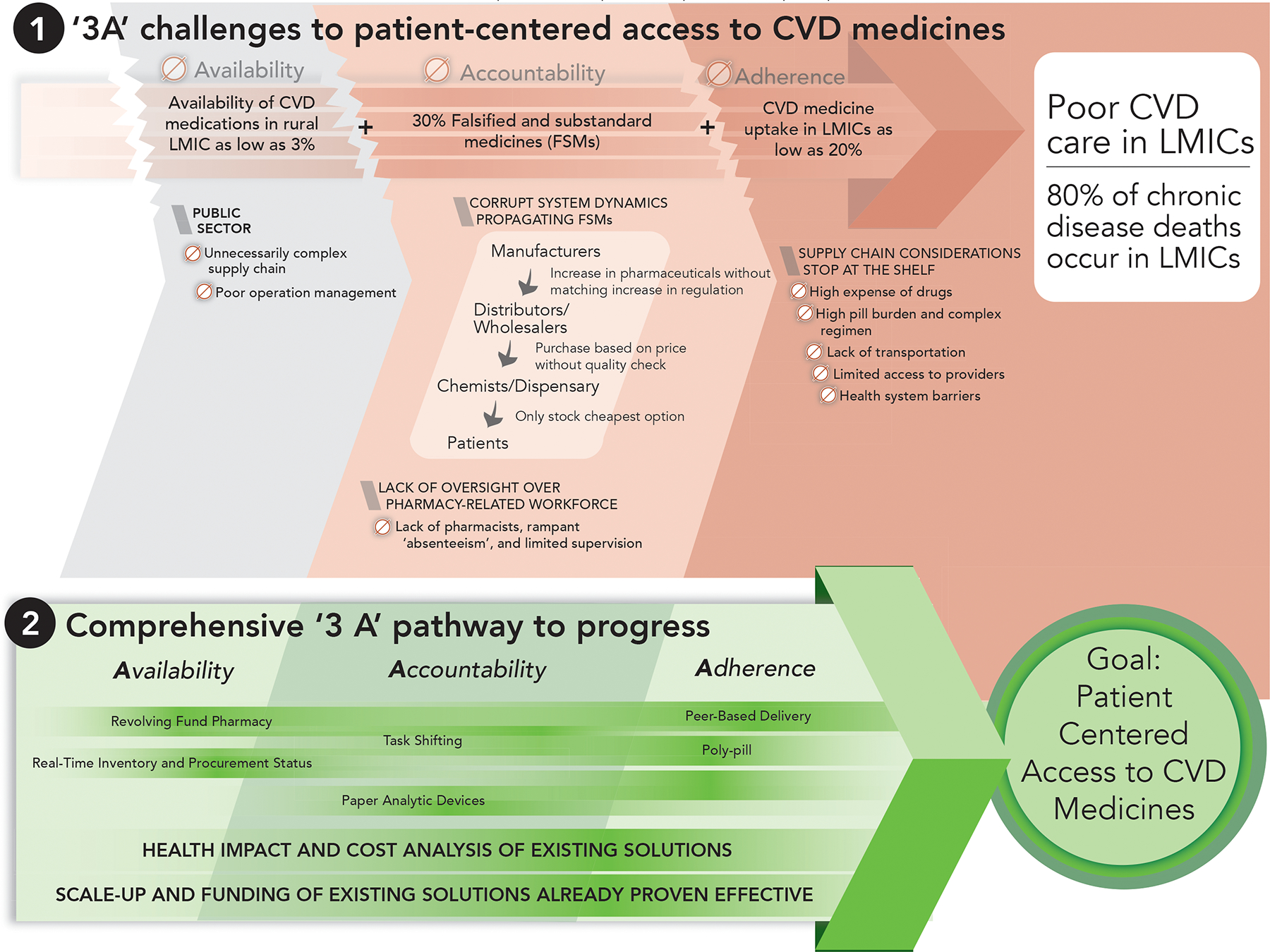
Cardiovascular disease (CVD) is the leading cause of global mortality and is expected to reach 23 million deaths by 2030. Eighty percent of CVD deaths occur in low-income and middle-income countries (LMICs). Although CVD prevention and treatment guidelines are available, translating these into practice is hampered in LMICs by inadequate health care systems that limit access to lifesaving medications. In this review article, we describe the deficiencies in the current LMIC supply chains that limit access to effective CVD medicines, and discuss existing solutions that are translatable to similar settings so as to address these deficiencies.
Keywords: Accountability; Adherence; Availability; Cardiovascular disease medicines; Falsified and substandard medicines; Health-system strengthening; Low-income and middle-income countries; Patient-centered access.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Dan N. Tran
Disclosure statement: The author does not have any commercial, financial conflicts of interests, or any funding sources to declare.
Benson Njuguna
Disclosure statement: The author does not have any commercial, financial conflicts of interests, or any funding sources to declare.
Timothy Mercer
Disclosure statement: The author does not have any commercial, financial conflicts of interests, or any funding sources to declare.
Imran Manji
Disclosure statement: The author does not have any commercial, financial conflicts of interests, or any funding sources to declare.
Lydia Fischer
Disclosure statement: The author does not have any commercial, financial conflicts of interests, or any funding sources to declare.
Marya Lieberman
Disclosure statement: The author has received funding for this project from the Bill & Melinda Gates Foundation, US-AID DIV program, and Indiana CTSI program.
Figures


References
-
- World Health Organization. Global status report on noncommunicable diseases 2014. Geneva: WHO; 2014. - PubMed
-
- Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation. 2001;104(22):2746–2753. - PubMed
-
- Fuster V, Kelly BB, Vedanthan R. Promoting Global Cardiovascular Health: Moving Forward. Circulation. 2011;123(15):1671–1678. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
