

Intravascular versus surface cooling for targeted temperature management after out-of-hospital cardiac arrest - an analysis of the TTM trial data
- PMID: 27887653
- PMCID: PMC5124238
- DOI: 10.1186/s13054-016-1552-6
Intravascular versus surface cooling for targeted temperature management after out-of-hospital cardiac arrest - an analysis of the TTM trial data
Abstract
Background: Targeted temperature management is recommended after out-of-hospital cardiac arrest and may be achieved using a variety of cooling devices. This study was conducted to explore the performance and outcomes for intravascular versus surface devices for targeted temperature management after out-of-hospital cardiac arrest.
Method: A retrospective analysis of data from the Targeted Temperature Management trial. N = 934. A total of 240 patients (26%) managed with intravascular versus 694 (74%) with surface devices. Devices were assessed for speed and precision during the induction, maintenance and rewarming phases in addition to adverse events. All-cause mortality, as well as a composite of poor neurological function or death, as evaluated by the Cerebral Performance Category and modified Rankin scale were analysed.
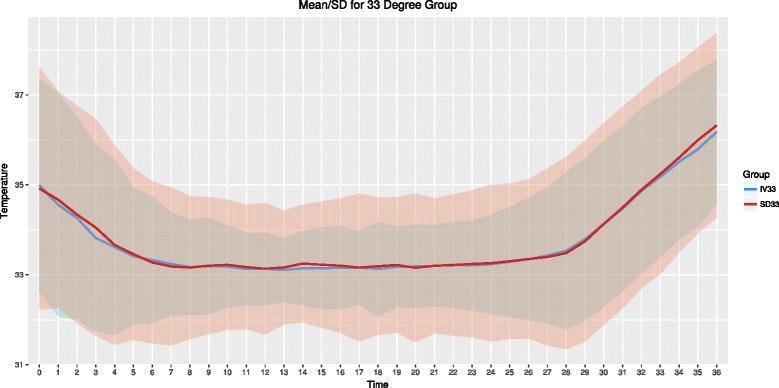
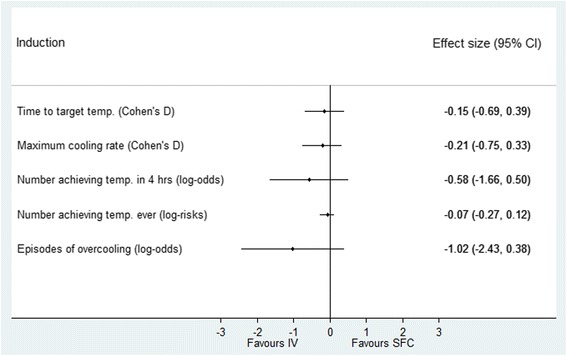
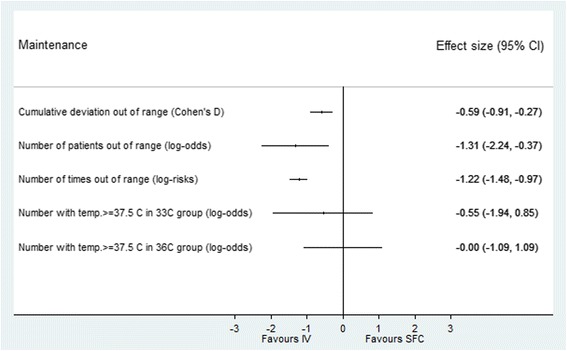
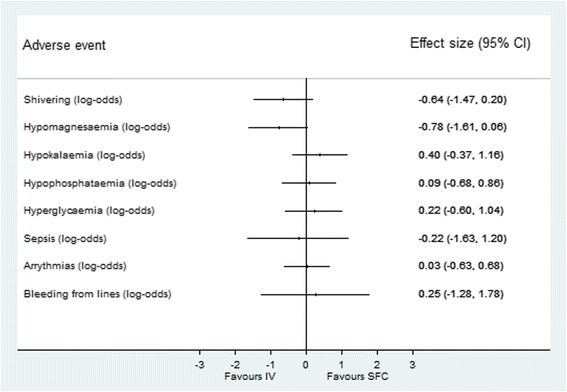
Results: For patients managed at 33 °C there was no difference between intravascular and surface groups in the median time taken to achieve target temperature (210 [interquartile range (IQR) 180] minutes vs. 240 [IQR 180] minutes, p = 0.58), maximum rate of cooling (1.0 [0.7] vs. 1.0 [0.9] °C/hr, p = 0.44), the number of patients who reached target temperature (within 4 hours (65% vs. 60%, p = 0.30); or ever (100% vs. 97%, p = 0.47), or episodes of overcooling (8% vs. 34%, p = 0.15). In the maintenance phase, cumulative temperature deviation (median 3.2 [IQR 5.0] °C hr vs. 9.3 [IQR 8.0] °C hr, p = <0.001), number of patients ever out of range (57.0% vs. 91.5%, p = 0.006) and median time out of range (1 [IQR 4.0] hours vs. 8.0 [IQR 9.0] hours, p = <0.001) were all significantly greater in the surface group although there was no difference in the occurrence of pyrexia. Adverse events were not different between intravascular and surface groups. There was no statistically significant difference in mortality (intravascular 46.3% vs. surface 50.0%; p = 0.32), Cerebral Performance Category scale 3-5 (49.0% vs. 54.3%; p = 0.18) or modified Rankin scale 4-6 (49.0% vs. 53.0%; p = 0.48).
Conclusions: Intravascular and surface cooling was equally effective during induction of mild hypothermia. However, surface cooling was associated with less precision during the maintenance phase. There was no difference in adverse events, mortality or poor neurological outcomes between patients treated with intravascular and surface cooling devices.
Trial registration: TTM trial ClinicalTrials.gov number https://clinicaltrials.gov/ct2/show/NCT01020916 NCT01020916; 25 November 2009.
Keywords: Brain injuries; Critical care; Fever; Hypothermia; Induced; Out-of-hospital cardiac arrest; Shivering; Temperature.
Figures

Comment in
-
Studies should fully report on variables that determine the dynamics and the temperature gradients during hypothermia.Crit Care. 2018 Sep 21;22(1):219. doi: 10.1186/s13054-018-2145-3. Crit Care. 2018. PMID: 30236138 Free PMC article. No abstract available.
Similar articles
-
Intravascular versus surface cooling for targeted temperature management after out-of-hospital cardiac arrest: an analysis of the TTH48 trial.Crit Care. 2019 Feb 22;23(1):61. doi: 10.1186/s13054-019-2335-7. Crit Care. 2019. PMID: 30795782 Free PMC article. Clinical Trial.
-
COOL-ARREST: Results from a Pilot Multicenter, Prospective, Single-Arm Observational Trial to Assess Intravascular Temperature Management in the Treatment of Cardiac Arrest.Ther Hypothermia Temp Manag. 2019 Mar;9(1):56-62. doi: 10.1089/ther.2018.0007. Epub 2018 Jun 8. Ther Hypothermia Temp Manag. 2019. PMID: 29883298
-
Endovascular Versus External Targeted Temperature Management for Patients With Out-of-Hospital Cardiac Arrest: A Randomized, Controlled Study.Circulation. 2015 Jul 21;132(3):182-93. doi: 10.1161/CIRCULATIONAHA.114.012805. Epub 2015 Jun 19. Circulation. 2015. PMID: 26092673 Clinical Trial.
-
What is the proper target temperature for out-of-hospital cardiac arrest?Best Pract Res Clin Anaesthesiol. 2015 Dec;29(4):425-34. doi: 10.1016/j.bpa.2015.09.003. Epub 2015 Sep 30. Best Pract Res Clin Anaesthesiol. 2015. PMID: 26670814 Review.
-
Targeted temperature management after out-of-hospital cardiac arrest: who, when, why, and how?Can Fam Physician. 2015 Feb;61(2):129-34. Can Fam Physician. 2015. PMID: 25821870 Free PMC article. Review.
Cited by
-
Target temperature management versus normothermia without temperature feedback systems for out-of-hospital cardiac arrest survivors.J Int Med Res. 2022 Sep;50(9):3000605221126880. doi: 10.1177/03000605221126880. J Int Med Res. 2022. PMID: 36177833 Free PMC article.
-
Targeted Temperature Management and Multimodality Monitoring of Comatose Patients After Cardiac Arrest.Front Neurol. 2018 Sep 11;9:768. doi: 10.3389/fneur.2018.00768. eCollection 2018. Front Neurol. 2018. PMID: 30254606 Free PMC article. Review.
-
Intravascular versus surface cooling for targeted temperature management after out-of-hospital cardiac arrest: an analysis of the TTH48 trial.Crit Care. 2019 Feb 22;23(1):61. doi: 10.1186/s13054-019-2335-7. Crit Care. 2019. PMID: 30795782 Free PMC article. Clinical Trial.
-
[Targeted temperature management after cardiac arrest : What is new?].Anaesthesist. 2022 Feb;71(2):85-93. doi: 10.1007/s00101-022-01091-1. Epub 2022 Jan 20. Anaesthesist. 2022. PMID: 35050390 German.
-
Targeted Temperature Management for Treatment of Cardiac Arrest.Curr Treat Options Cardiovasc Med. 2020;22(11):39. doi: 10.1007/s11936-020-00846-6. Epub 2020 Oct 10. Curr Treat Options Cardiovasc Med. 2020. PMID: 33071538 Free PMC article. Review.
References
-
- Arrich J, Holzer M, Havel C, Müllner M, Herkner H. Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation. Cochrane Database Syst Rev 2012, Issue 9. Art. No.: CD004128. doi:10.1002/14651858.CD004128.pub3 - PubMed
-
- Uray T, Sterz F, Janata A, et al. Surface cooling with a new cooling-blanket for rapid induction of mild hypothermia in humans after cardiac arrest: a feasibility trial. Resuscitation. 2006;69:93.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
