

Evaluating the Four Kallikrein Panel of the 4Kscore for Prediction of High-grade Prostate Cancer in Men in the Canary Prostate Active Surveillance Study
- PMID: 27889277
- PMCID: PMC7327706
- DOI: 10.1016/j.eururo.2016.11.017
Evaluating the Four Kallikrein Panel of the 4Kscore for Prediction of High-grade Prostate Cancer in Men in the Canary Prostate Active Surveillance Study
Abstract
Background: Diagnosis of Gleason 6 prostate cancer can leave uncertainty about the presence of undetected aggressive disease.
Objective: To evaluate the utility of a four kallikrein (4K) panel in predicting the presence of high-grade cancer in men on active surveillance.
Design, setting, and participants: Plasma collected before the first and subsequent surveillance biopsies was assessed for 718 men prospectively enrolled in the multi-institutional Canary PASS trial. Biopsy data were split 2:1 into training and test sets. We developed statistical models that included clinical information and either the 4Kpanel or serum prostate-specific antigen (PSA).
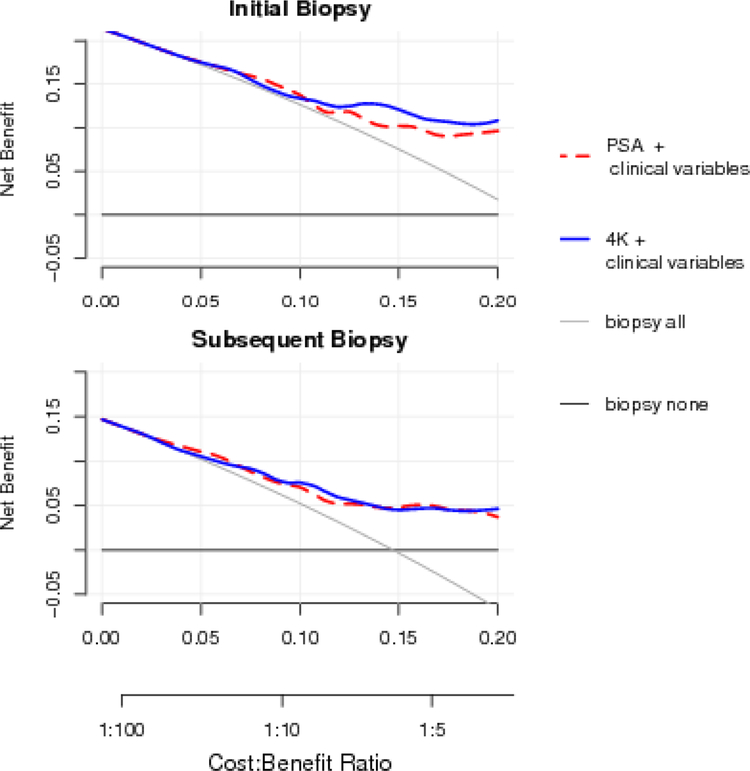
Outcome measurements and statistical analysis: The endpoint was reclassification to Gleason ≥7. We used receiver operating characteristic (ROC) curve analyses and area under the curve (AUC) to assess discriminatory capacity, and decision curve analysis (DCA) to report clinical net benefit.
Results and limitations: Significant predictors for reclassification were 4Kpanel (odds ratio [OR] 1.54, 95% confidence interval [CI] 1.31-1.81) or PSA (OR 2.11, 95% CI 1.53-2.91), ≥20% cores positive (OR 2.10, 95% CI 1.33-3.32), two or more prior negative biopsies (OR 0.19, 95% CI 0.04-0.85), prostate volume (OR 0.47, 95% CI 0.31-0.70), and body mass index (OR 1.09, 95% CI 1.04-1.14). ROC curve analysis comparing 4K and base models indicated that the 4Kpanel improved accuracy for predicting reclassification (AUC 0.78 vs 0.74) at the first surveillance biopsy. Both models performed comparably for prediction of reclassification at subsequent biopsies (AUC 0.75 vs 0.76). In DCA, both models showed higher net benefit compared to biopsy-all and biopsy-none strategies. Limitations include the single cohort nature of the study and the small numbers; results should be validated in another cohort before clinical use.
Conclusions: The 4Kpanel provided incremental value over routine clinical information in predicting high-grade cancer in the first biopsy after diagnosis. The 4Kpanel did not add predictive value to the base model at subsequent surveillance biopsies.
Patient summary: Active surveillance is a management strategy for many low-grade prostate cancers. Repeat biopsies monitor for previously undetected high-grade cancer. We show that a model with clinical variables, including a panel of four kallikreins, indicates the presence of high-grade cancer before a biopsy is performed.
Keywords: Active surveillance; Biomarker; Kallikrein; Prospective studies; Prostatic neoplasms.
Copyright © 2016 European Association of Urology. All rights reserved.
Conflict of interest statement
Figures
References
-
- Parekh DJ, Punnen S, Sjoberg DD, et al. A multi-institutional prospective trial in the USA confirms that the 4Kscore accurately identifies men with high-grade prostate cancer. Eur Urol 2015;68:464–70. - PubMed
-
- Pan W Akaike’s information criterion in generalized estimating equations. Biometrics 2001;57:120–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
